

Esophagogastric junction distensibility measurements during Heller myotomy and POEM for achalasia predict postoperative symptomatic outcomes
- PMID: 25055891
- PMCID: PMC4343529
- DOI: 10.1007/s00464-014-3733-1
Esophagogastric junction distensibility measurements during Heller myotomy and POEM for achalasia predict postoperative symptomatic outcomes
Abstract
Background: The functional lumen imaging probe (FLIP) is a novel diagnostic tool that can be used to measure esophagogastric junction (EGJ) distensibility. In this study, we performed intraoperative FLIP measurements during laparoscopic Heller myotomy (LHM) and peroral esophageal myotomy (POEM) for treatment of achalasia and evaluated the relationship between EGJ distensibility and postoperative symptoms.
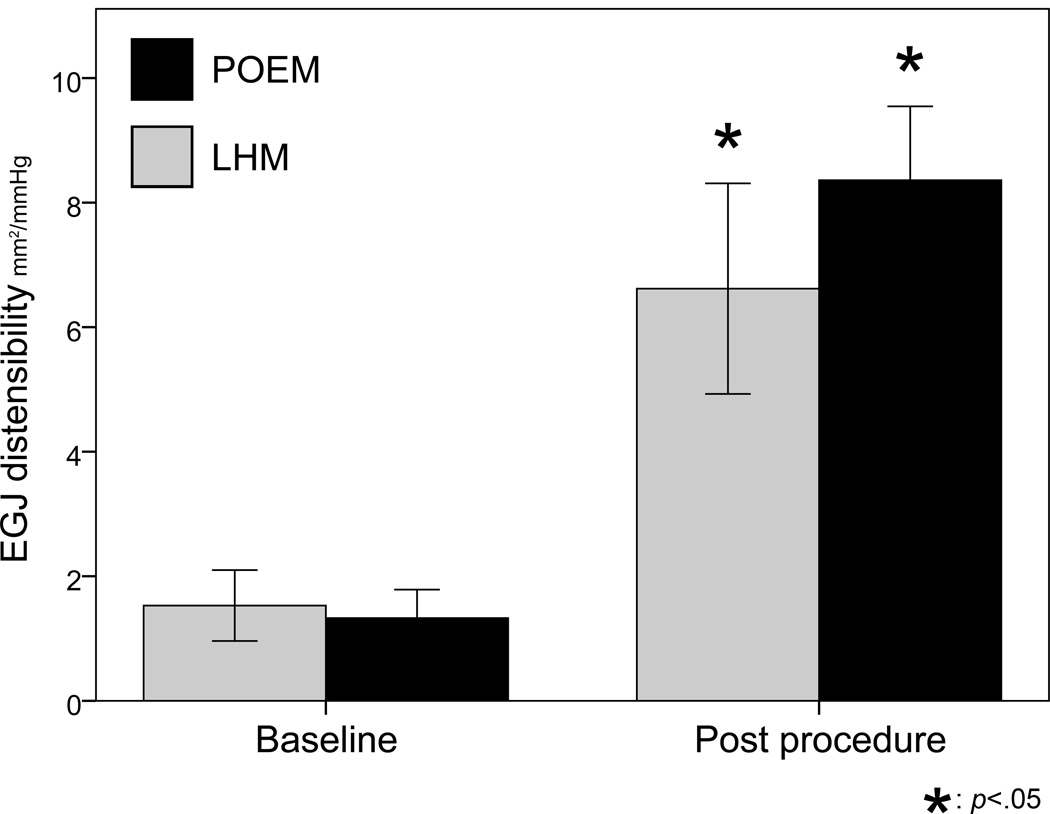
Methods: Distensibility index (DI) (defined as the minimum cross-sectional area at the EGJ divided by distensive pressure) was measured with FLIP at two time points during LHM and POEM: (1) at baseline after induction of anesthesia, and (2) after operation completion.
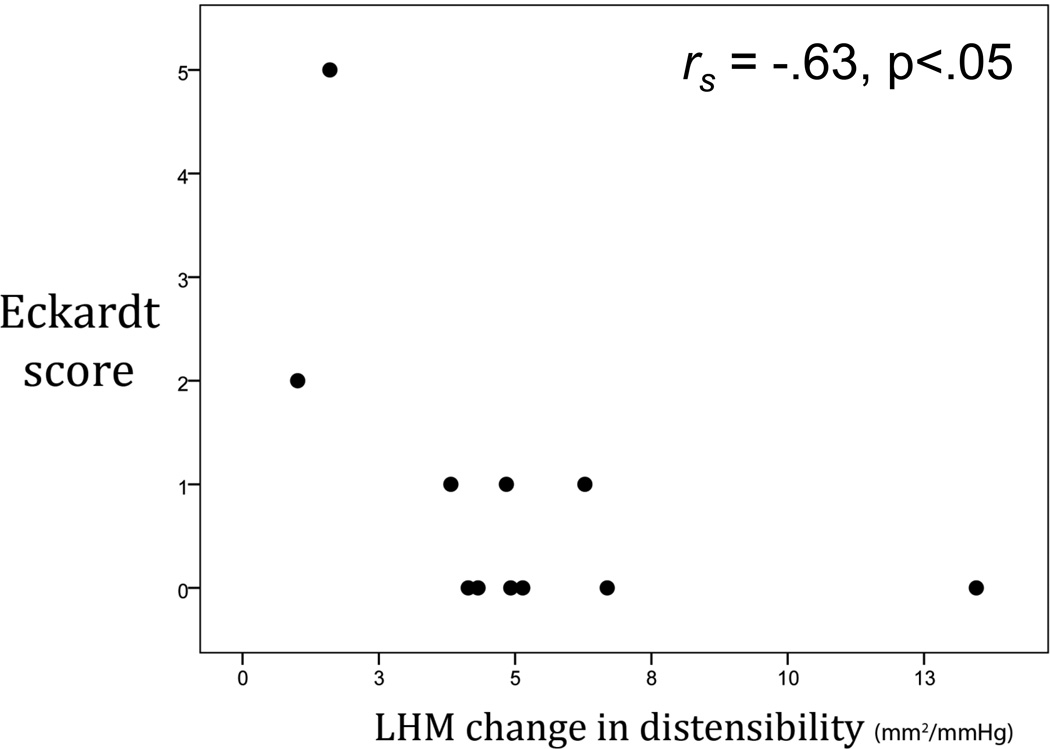
Results: Measurements were performed in 20 patients undergoing LHM and 36 undergoing POEM. Both operations resulted in an increase in DI, although this increase was larger with POEM (7 ± 3.1 vs. 5.1 ± 3.4 mm(2)/mmHg, p < .05). The two patients (both LHM) with the smallest increases in DI (1 and 1.6 mm(2)/mmHg) both had persistent symptoms postoperatively and, overall, LHM patients with larger increases in DI had lower postoperative Eckardt scores. In the POEM group, there was no correlation between change in DI and symptoms; however, all POEM patients experienced an increase in DI of >3 mm(2)/mmHg. When all patients were divided into thirds based on final DI, none in the lowest DI group (<6 mm(2)/mmHg) had symptoms suggestive of reflux (i.e., GerdQ score >7), as compared with 20 % in the middle third (6-9 mm(2)/mmHg) and 36 % in the highest third (>9 mm(2)/mmHg). Patients within an "ideal" final DI range (4.5-8.5 mm(2)/mmHg) had optimal symptomatic outcomes (i.e., Eckardt ≤ 1 and GerdQ ≤ 7) in 88 % of cases, compared with 47 % in those with a final DI above or below that range (p < .05).
Conclusions: Intraoperative EGJ distensibility measurements with FLIP were predictive of postoperative symptomatic outcomes. These results provide initial evidence that FLIP has the potential to act as a useful calibration tool during operations for achalasia.
Figures
References
-
- Triadafilopoulos G, Boeckxstaens GE, Gullo R, Patti MG, Pandolfino JE, Kahrilas PJ, Duranceau A, Jamieson G, Zaninotto G. The Kagoshima consensus on esophageal achalasia. Dis Esophagus. 2012;25:337–348. - PubMed
-
- Boeckxstaens GE, Annese V, des Varannes SB, Chaussade S, Costantini M, Cuttitta A, Elizalde JI, Fumagalli U, Gaudric M, Rohof WO, Smout AJ, Tack J, Zwinderman AH, Zaninotto G, Busch OR, European Achalasia Trial I. Pneumatic dilation versus laparoscopic Heller's myotomy for idiopathic achalasia. N Engl J Med. 2011;364:1807–1816. - PubMed
-
- Campos GM, Vittinghoff E, Rabl C, Takata M, Gadenstatter M, Lin F, Ciovica R. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg. 2009;249:45–57. - PubMed
-
- Yaghoobi M, Mayrand S, Martel M, Roshan-Afshar I, Bijarchi R, Barkun A. Laparoscopic Heller’s myotomy versus pneumatic dilation in the treatment of idiopathic achalasia: a meta-analysis of randomized, controlled trials. Gastrointest Endosc. 2013;78:468–475. - PubMed
-
- Novais PA, Lemme EM. 24-h pH monitoring patterns and clinical response after achalasia treatment with pneumatic dilation or laparoscopic Heller myotomy. Aliment Pharmacol Ther. 2010;32:1257–1265. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
