

Sexual bother in men with advanced prostate cancer undergoing androgen deprivation therapy
- PMID: 25059094
- PMCID: PMC11302979
- DOI: 10.1111/jsm.12645
Sexual bother in men with advanced prostate cancer undergoing androgen deprivation therapy
Abstract
Introduction: Men with advanced prostate cancer (APC) undergoing androgen deprivation therapy (ADT) often experience distressing sexual side effects. Sexual bother is an important component of adjustment. Factors associated with increased bother are not well understood.
Aims: This study sought to describe sexual dysfunction and bother in APC patients undergoing ADT, identify socio-demographic and health/disease-related characteristics related to sexual bother, and evaluate associations between sexual bother and psychosocial well-being and quality of life (QOL).
Methods: Baseline data of a larger psychosocial intervention study was used. Pearson's correlation and independent samples t-test tested bivariate relations. Multivariate regression analysis evaluated relations between sexual bother and psychosocial and QOL outcomes.
Main outcome measures: The Expanded Prostate Cancer Index Composite sexual function and bother subscales, Center for Epidemiologic Studies Depression Scale, Functional Assessment of Cancer Therapy--General, and Dyadic Adjustment Scale were the main outcome measures.
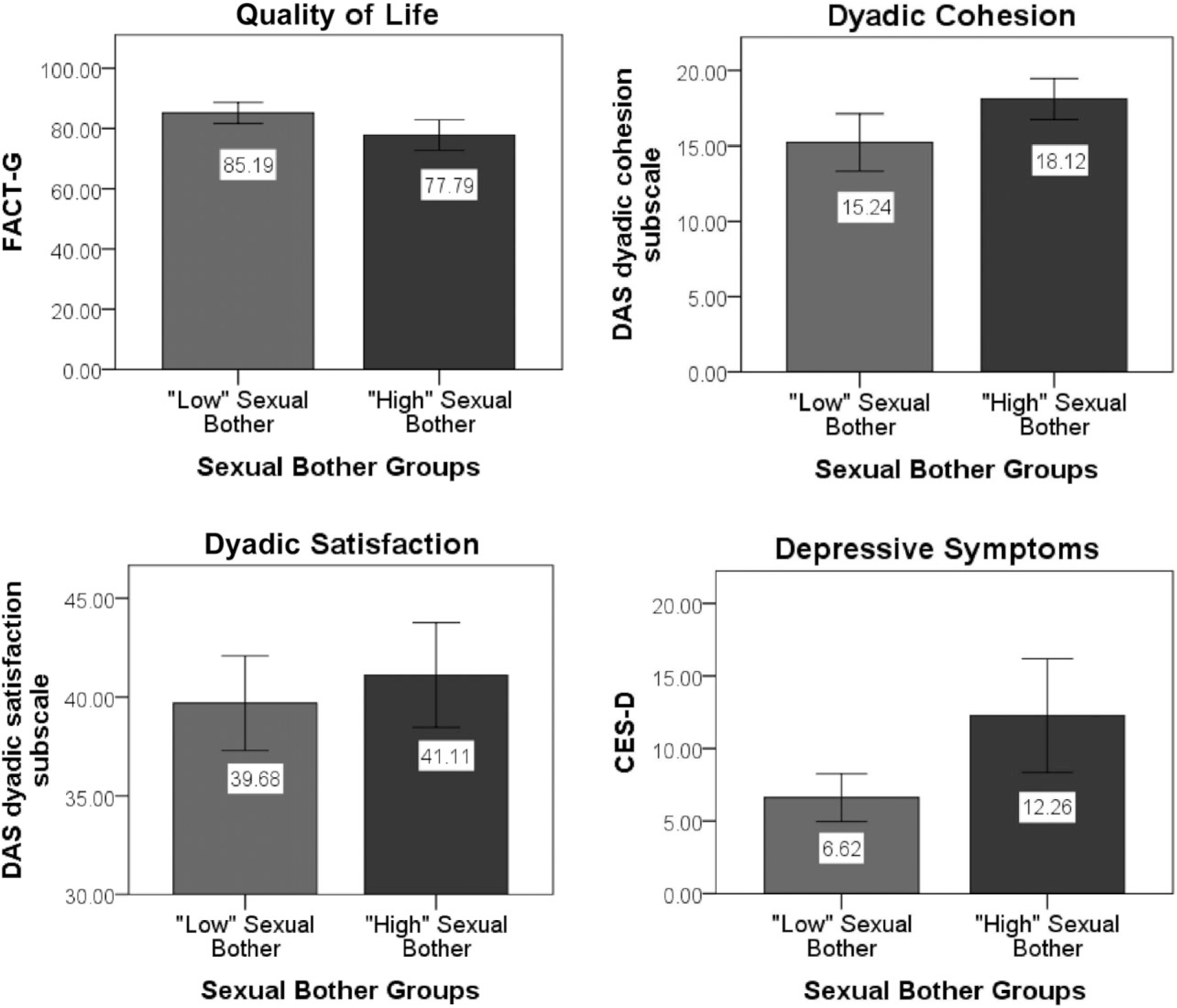
Results: Participants (N = 80) were 70 years old (standard deviation [SD] = 9.6) and reported 18.7 months (SD = 17.3) of ADT. Sexual dysfunction (mean = 10.1; SD = 18.0) was highly prevalent. Greater sexual bother (lower scores) was related to younger age (β = 0.25, P = 0.03) and fewer months of ADT (β = 0.22, P = 0.05). Controlling for age, months of ADT, current and precancer sexual function, sexual bother correlated with more depressive symptoms (β = -0.24, P = 0.06) and lower QOL (β = 0.25, P = 0.05). Contrary to hypotheses, greater sexual bother was related to greater dyadic satisfaction (β = -0.35, P = 0.03) and cohesion (β = -0.42, P = 0.01).
Conclusions: The majority of APC patients undergoing ADT will experience sexual dysfunction, but there is variability in their degree of sexual bother. Psychosocial aspects of sexual functioning should be considered when evaluating men's adjustment to ADT effects. Assessment of sexual bother may help identify men at risk for more general distress and lowered QOL. Psychosocial interventions targeting sexual bother may complement medical treatments for sexual dysfunction and be clinically relevant, particularly for younger men and those first starting ADT.
Keywords: Androgen Ablation; Androgen Deprivation; Depressive Symptoms; Erectile Dysfunction; Hormone Therapy; Prostate Cancer; Quality of Life; Relationship Functioning; Sexual Bother; Sexual Dysfunction; Sexual Function.
© 2014 International Society for Sexual Medicine.
Conflict of interest statement
Figures
References
-
- Gomella LG. Contemporary use of hormonal therapy in prostate cancer: Managing complications and addressing quality-of-life issues. BJU Int 2007;99(suppl 1):25–9, discussion 30. - PubMed
-
- Roach M Current trends for the use of androgen deprivation therapy in conjunction with radiotherapy for patients with unfavorable intermediate-risk, high-risk, localized, and locally advanced prostate cancer. Cancer 2014;120:1620–9. - PubMed
-
- Bastian PJ, Boorjian SA, Bossi A, Briganti A, Heidenreich A, Freedland SJ, Montorsi F, Roach Iii M, Schröder F, van Poppel H, Stief CG, Stephenson AJ, Zelefsky MJ. High-risk prostate cancer: From definition to contemporary management. Eur Urol 2012;61:1096–106. - PubMed
-
- American Cancer Society. Hormone (androgen deprivation) therapy for prostate cancer. American Cancer Society. 2013. Available at: http://www.cancer.org/cancer/prostatecancer/detailedguide/prostate-cance... (accessed October 22, 2013).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
