

Does neoadjuvant therapy for esophageal cancer increase postoperative morbidity or mortality?
- PMID: 25059343
- PMCID: PMC4324382
- DOI: 10.1111/dote.12251
Does neoadjuvant therapy for esophageal cancer increase postoperative morbidity or mortality?
Abstract
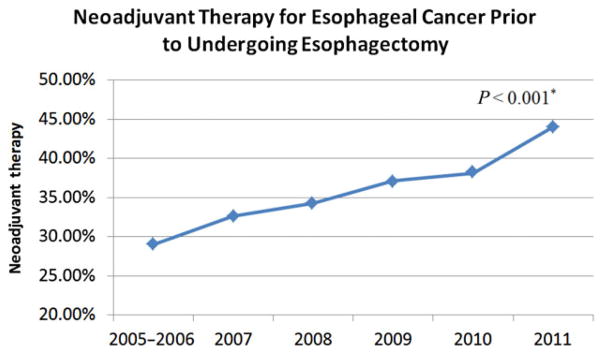
Neoadjuvant therapy has proven to be effective in the reduction of locoregional recurrence and mortality for esophageal cancer. However, induction treatment has been reported to be associated with increased risk of postoperative complications. We therefore compared outcomes after esophagectomy for esophageal cancer for patients who underwent neoadjuvant therapy and patients treated with surgery alone. Using the American College of Surgeons National Surgical Quality Improvement Program database (2005-2011), we identified 1939 patients who underwent esophagectomy for esophageal cancer. Seven hundred and eight (36.5%) received neoadjuvant therapy, while 1231 (63.5%) received no neoadjuvant therapy within 90 days prior to surgery. Primary outcome was 30-day mortality, and secondary outcomes included overall and serious morbidity, length of stay, and operative time. Patients who underwent neoadjuvant treatment were younger (62.3 vs. 64.7, P < 0.001), were more likely to have experienced recent weight loss (29.4% vs. 15.9%, P < 0.001), and had worse preoperative hematological cell counts (white blood cells <4.5 or >11 × 10(9) /L: 29.3% vs. 15.0%, P < 0.001; hematocrit <36%: 49.7% vs. 30.0%, P < 0.001). On unadjusted analysis, 30-day mortality, overall, and serious morbidity were comparable between the two groups, with the exception of the individual complications of venous thromboembolic events and bleeding transfusion, which were significantly lower in the surgery-only patients (5.71% vs. 8.27%, P = 0.027; 6.89% vs. 10.57%, P = 0.004; respectively). Multivariable and matched analysis confirmed that 30-day mortality, overall, and serious morbidity, as well as prolonged length of stay, were comparable between the two groups of patients. An increasing trend of preoperative neoadjuvant therapy for esophageal cancer was observed through the study years (from 29.0% in 2005-2006 to 44.0% in 2011, P < 0.001). According to our analysis, preoperative neoadjuvant therapy for esophageal cancer does not increase 30-day mortality or the overall risk of postoperative complications after esophagectomy.
Keywords: chemotherapy; esophageal cancer; esophagectomy; outcome; radiation therapy.
© 2014 International Society for Diseases of the Esophagus.
Figures
References
-
- International Agency for Research on Cancer. Oesophageal cancer: estimated incidence, mortality and prevalence worldwide in 2012. [Cited 9 Jan 2014.] Available from URL: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
-
- Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol. 2009;27:5062–7. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
