

Differential responses of osteoblasts and macrophages upon Staphylococcus aureus infection
- PMID: 25059520
- PMCID: PMC4116603
- DOI: 10.1186/s12866-014-0207-5
Differential responses of osteoblasts and macrophages upon Staphylococcus aureus infection
Abstract
Background: Staphylococcus aureus (S. aureus) is one of the primary causes of bone infections which are often chronic and difficult to eradicate. Bacteria like S. aureus may survive upon internalization in cells and may be responsible for chronic and recurrent infections. In this study, we compared the responses of a phagocytic cell (i.e. macrophage) to a non-phagocytic cell (i.e. osteoblast) upon S. aureus internalization.
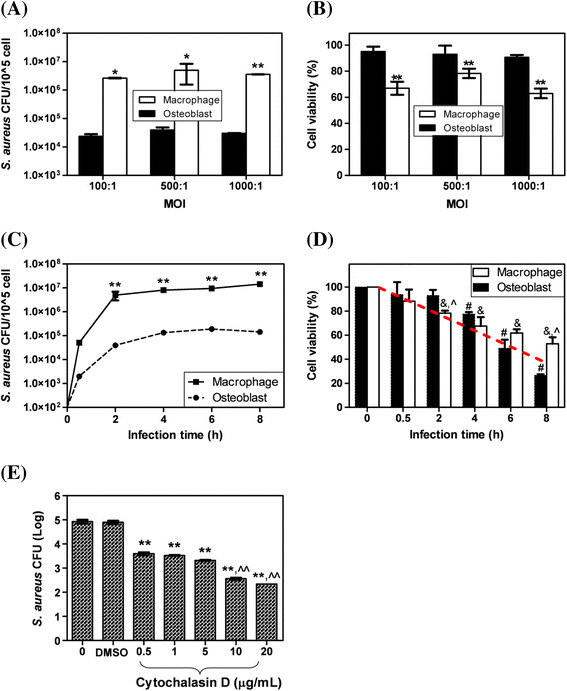
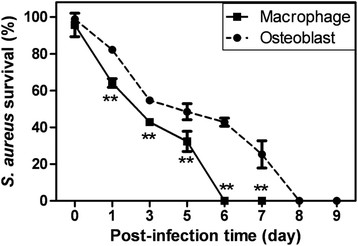
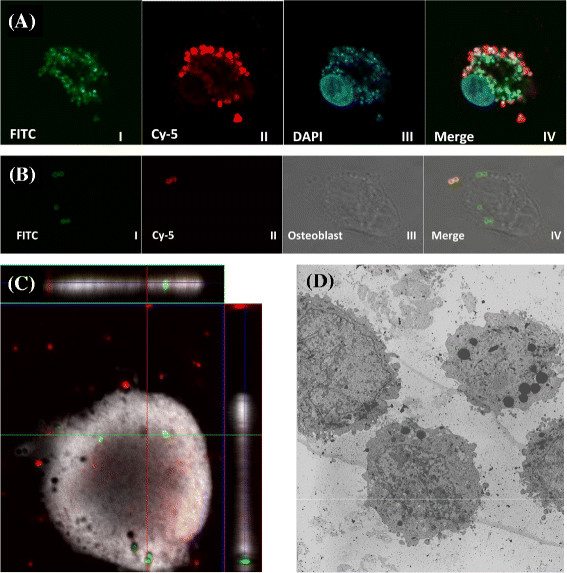
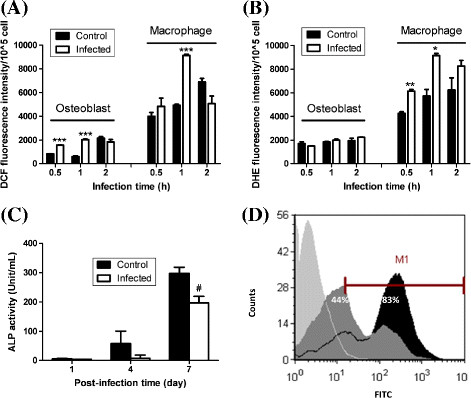
Results: We found that upon internalization, S. aureus could survive for up to 5 and 7 days within macrophages and osteoblasts, respectively. Significantly more S. aureus was internalized in macrophages compared to osteoblasts and a significantly higher (100 fold) level of live intracellular S. aureus was detected in macrophages compared to osteoblasts. However, the percentage of S. aureus survival after infection was significantly lower in macrophages compared to osteoblasts at post-infection days 1-6. Interestingly, macrophages had relatively lower viability in shorter infection time periods (i.e. 0.5-4 h; significant at 2 h) but higher viability in longer infection time periods (i.e. 6-8 h; significant at 8 h) compared to osteoblasts. In addition, S. aureus infection led to significant changes in reactive oxygen species production in both macrophages and osteoblasts. Moreover, infected osteoblasts had significantly lower alkaline phosphatase activity at post-infection day 7 and infected macrophages had higher phagocytosis activity compared to non-infected cells.
Conclusions: S. aureus was found to internalize and survive within osteoblasts and macrophages and led to differential responses between osteoblasts and macrophages. These findings may assist in evaluation of the pathogenesis of chronic and recurrent infections which may be related to the intracellular persistence of bacteria within host cells.
Figures
References
-
- von Eiff C, Becker K, Metze D, Lubritz G, Hockmann J, Schwarz T, Peters G. Intracellular persistence of Staphylococcus aureus small-colony variants within keratinocytes: A cause for antibiotic treatment failure in a patient with Darier’s disease. Clin Infect Dis. 2001;32(11):1643–1647. doi: 10.1086/320519. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
