

Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013
- PMID: 25059949
- PMCID: PMC4202387
- DOI: 10.1016/S0140-6736(14)60844-8
Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013
Erratum in
- Lancet. 2014 Oct 25;384(9953):1504
- Lancet. 2014 Sep 13;384(9947):956
Abstract
Background: The Millennium Declaration in 2000 brought special global attention to HIV, tuberculosis, and malaria through the formulation of Millennium Development Goal (MDG) 6. The Global Burden of Disease 2013 study provides a consistent and comprehensive approach to disease estimation for between 1990 and 2013, and an opportunity to assess whether accelerated progress has occured since the Millennium Declaration.
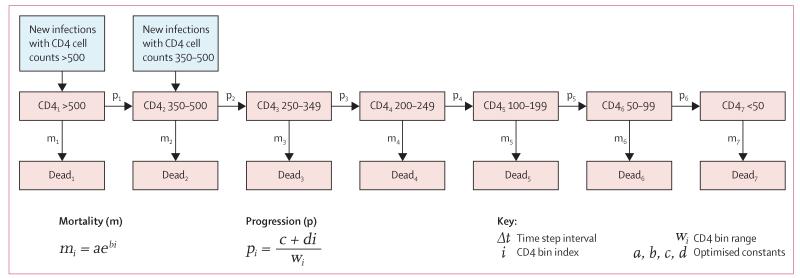
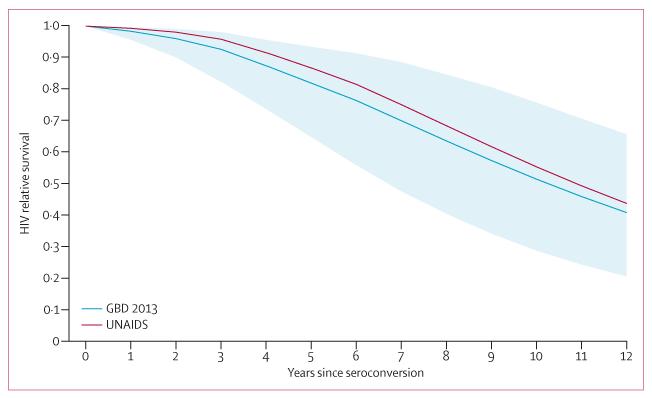
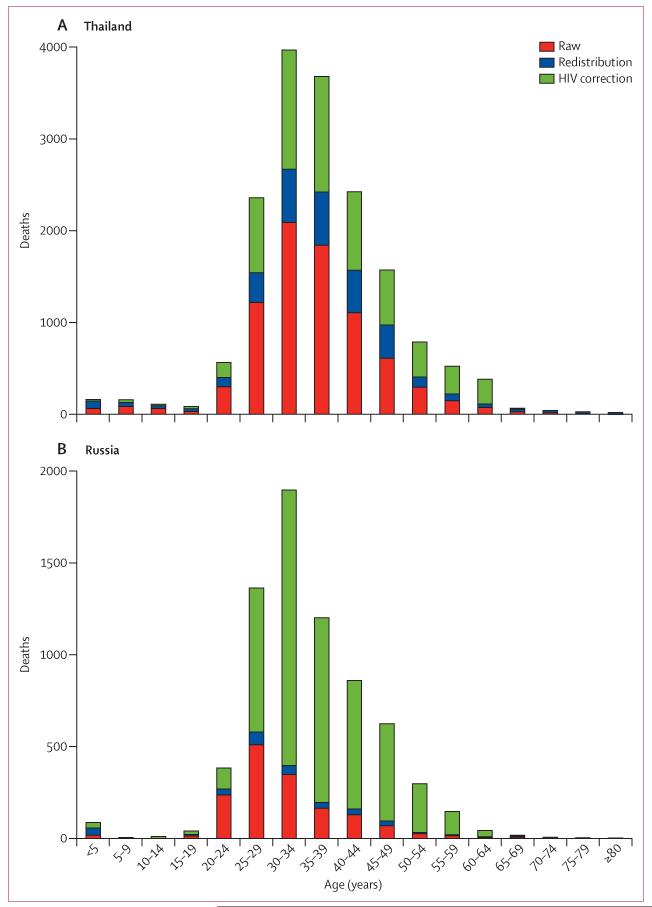
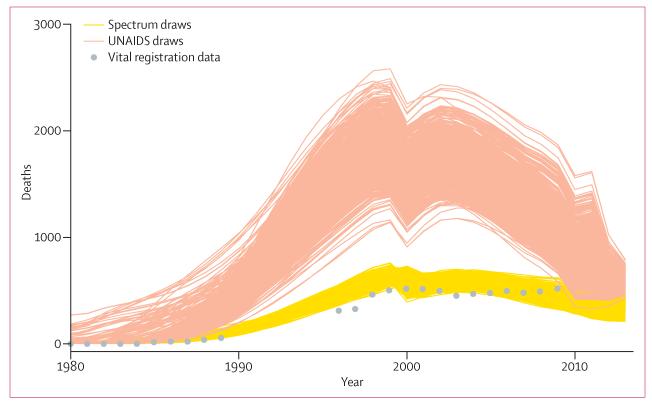
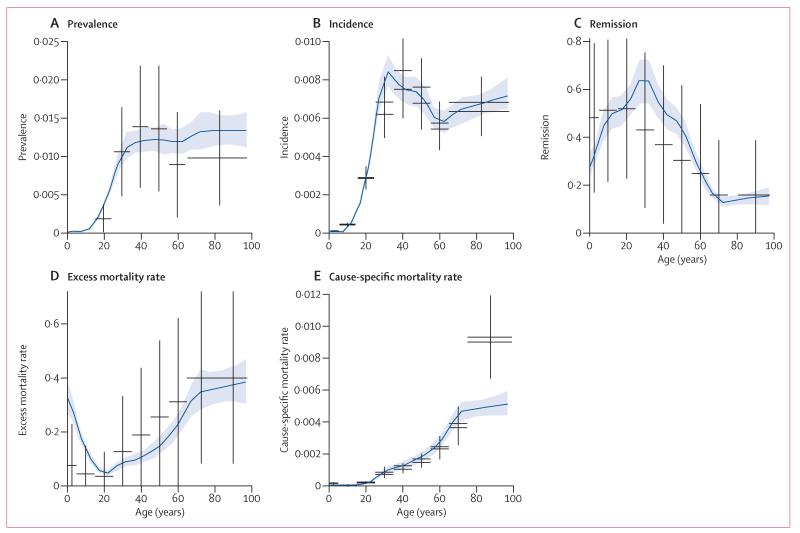
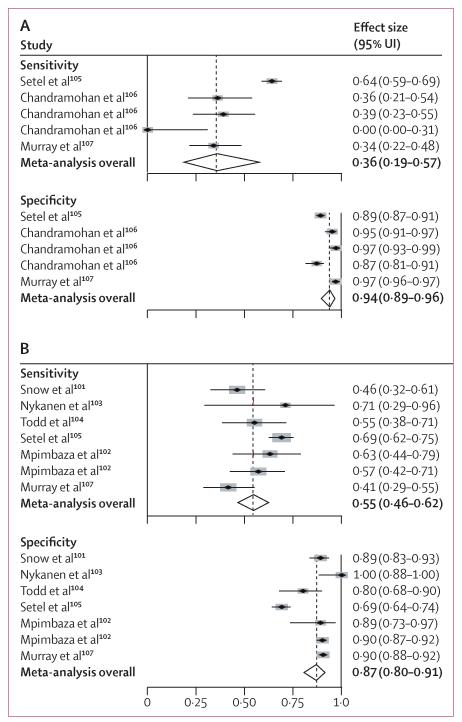
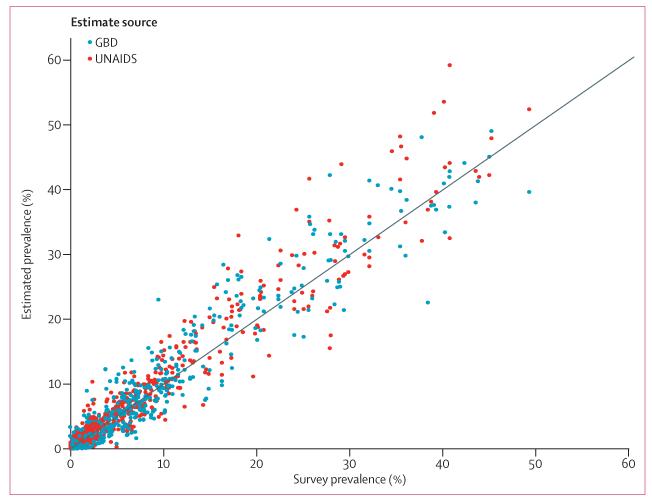
Methods: To estimate incidence and mortality for HIV, we used the UNAIDS Spectrum model appropriately modified based on a systematic review of available studies of mortality with and without antiretroviral therapy (ART). For concentrated epidemics, we calibrated Spectrum models to fit vital registration data corrected for misclassification of HIV deaths. In generalised epidemics, we minimised a loss function to select epidemic curves most consistent with prevalence data and demographic data for all-cause mortality. We analysed counterfactual scenarios for HIV to assess years of life saved through prevention of mother-to-child transmission (PMTCT) and ART. For tuberculosis, we analysed vital registration and verbal autopsy data to estimate mortality using cause of death ensemble modelling. We analysed data for corrected case-notifications, expert opinions on the case-detection rate, prevalence surveys, and estimated cause-specific mortality using Bayesian meta-regression to generate consistent trends in all parameters. We analysed malaria mortality and incidence using an updated cause of death database, a systematic analysis of verbal autopsy validation studies for malaria, and recent studies (2010-13) of incidence, drug resistance, and coverage of insecticide-treated bednets.
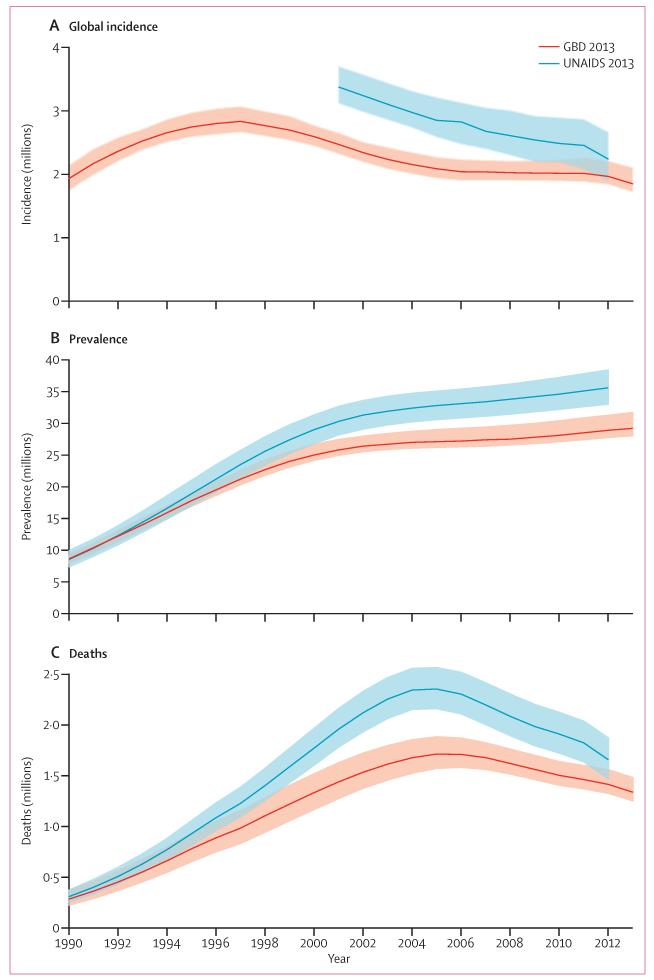
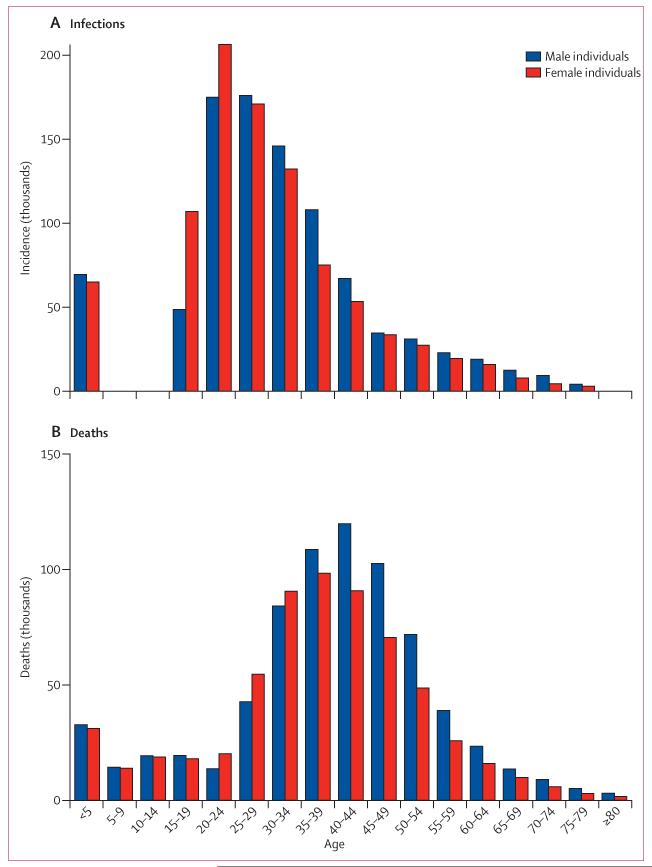
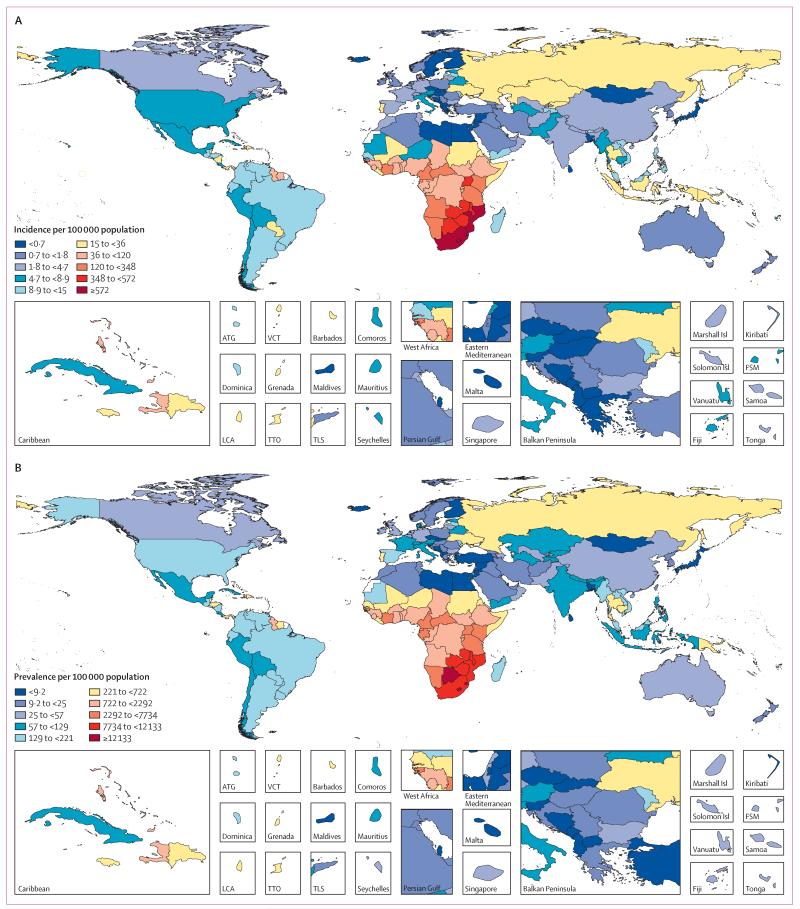
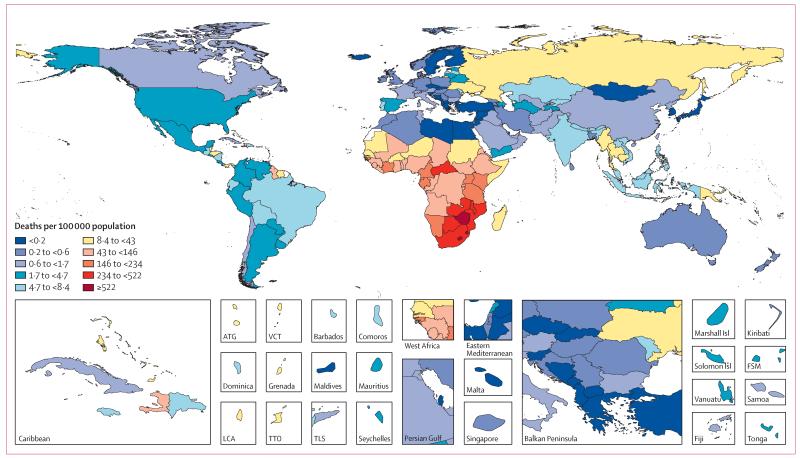
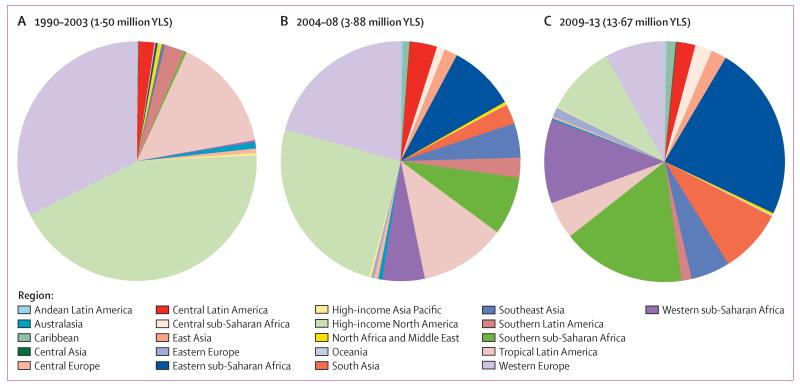
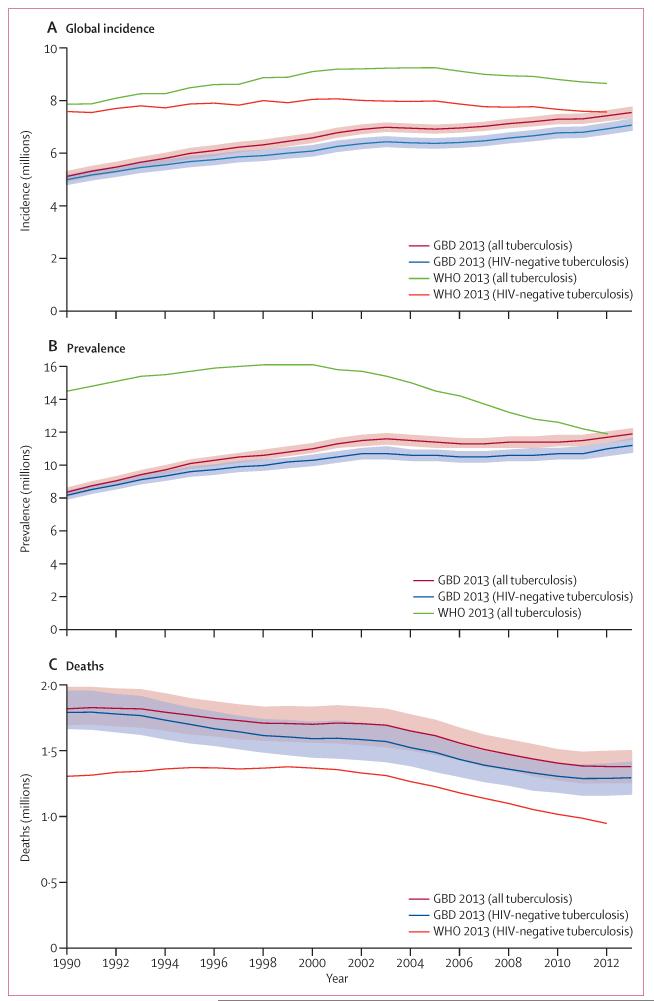
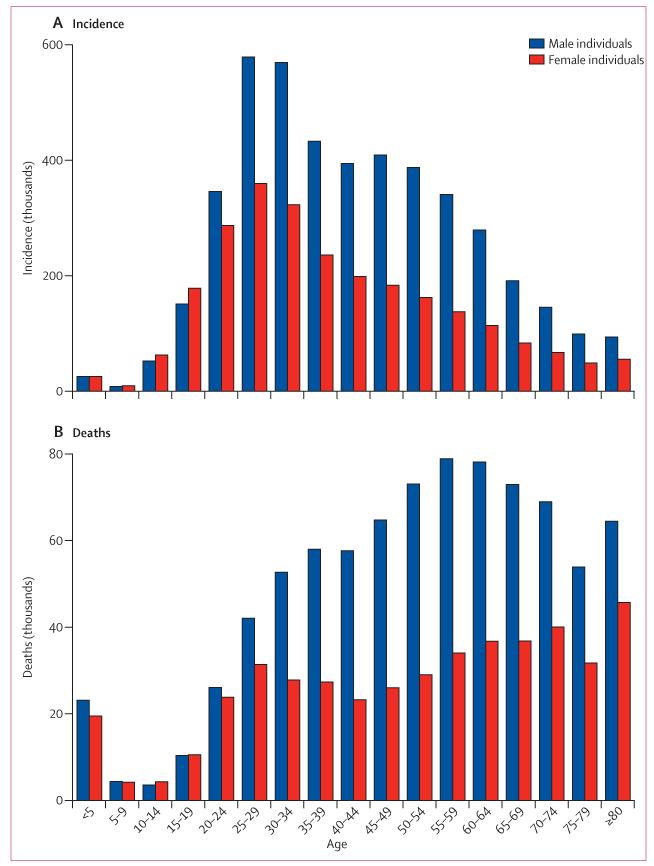
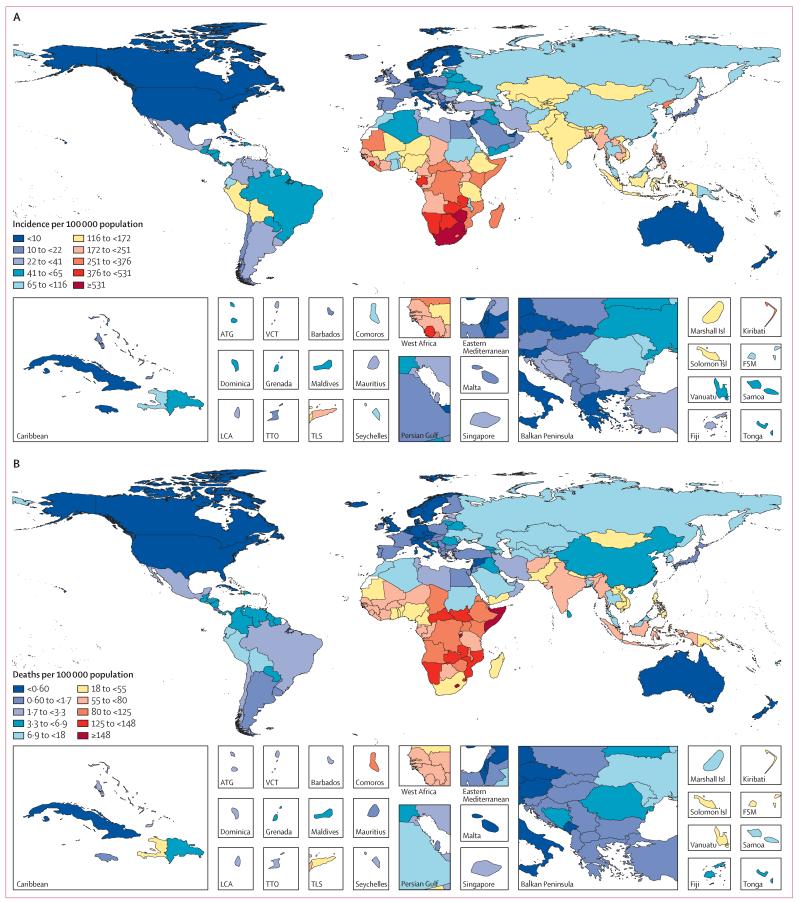
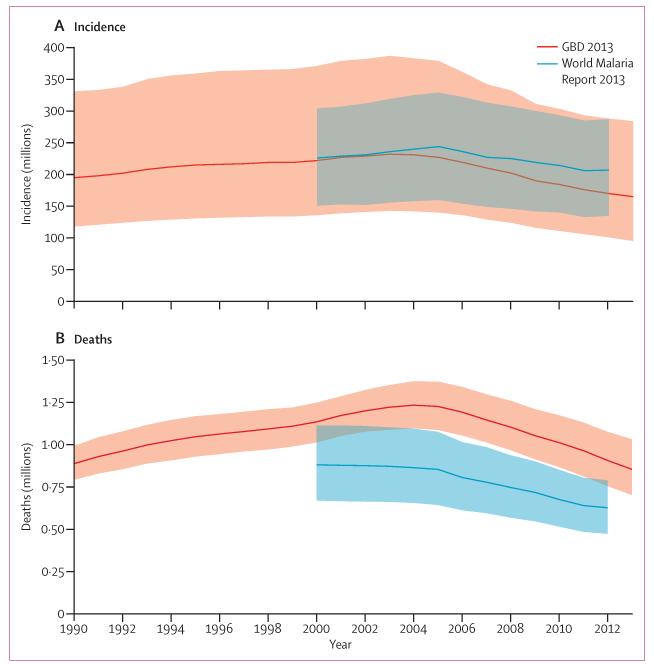
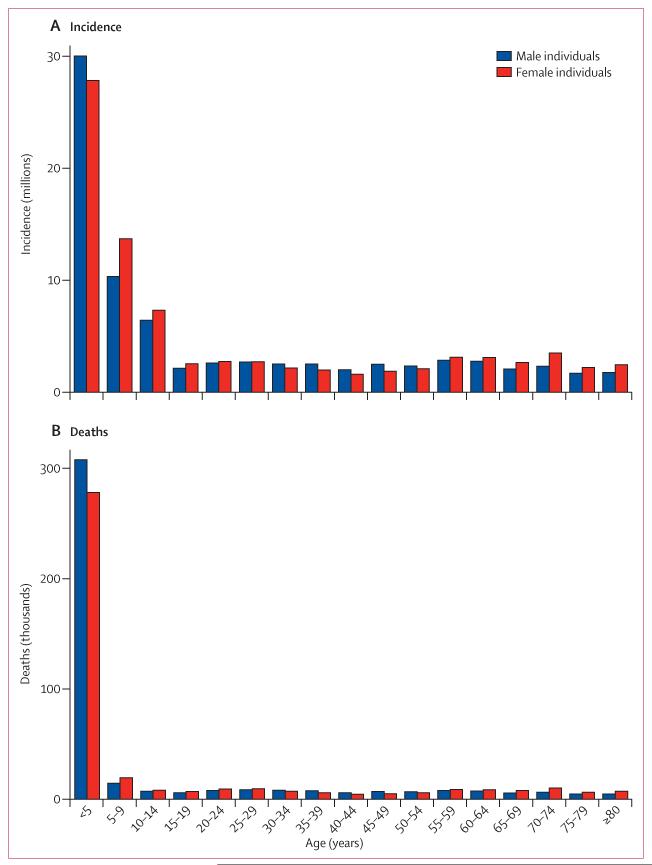
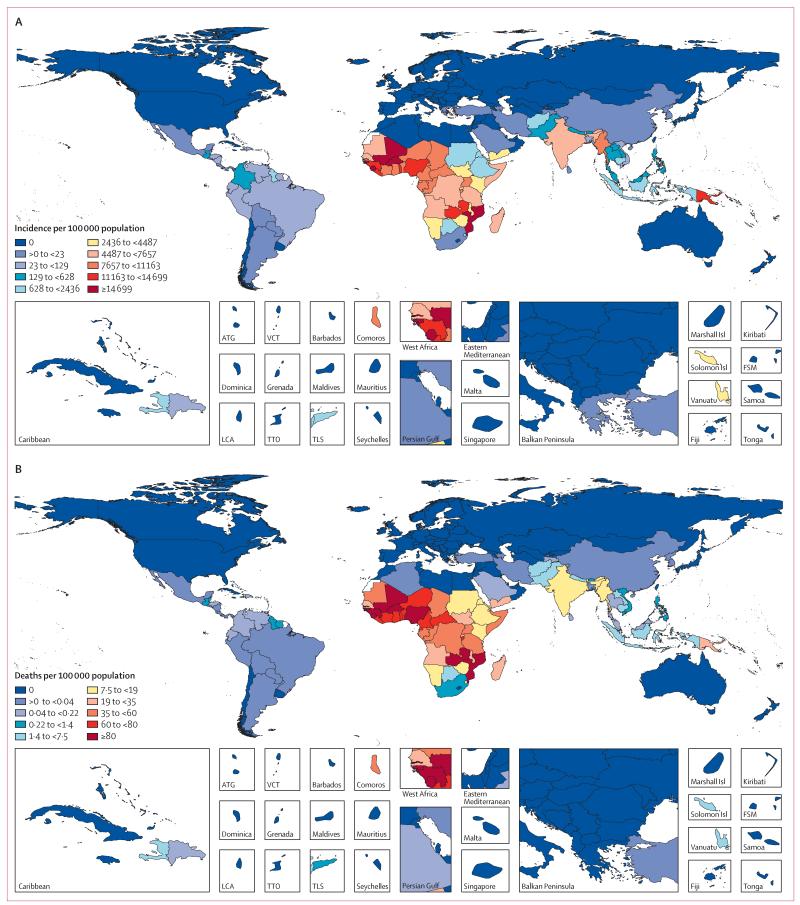
Findings: Globally in 2013, there were 1·8 million new HIV infections (95% uncertainty interval 1·7 million to 2·1 million), 29·2 million prevalent HIV cases (28·1 to 31·7), and 1·3 million HIV deaths (1·3 to 1·5). At the peak of the epidemic in 2005, HIV caused 1·7 million deaths (1·6 million to 1·9 million). Concentrated epidemics in Latin America and eastern Europe are substantially smaller than previously estimated. Through interventions including PMTCT and ART, 19·1 million life-years (16·6 million to 21·5 million) have been saved, 70·3% (65·4 to 76·1) in developing countries. From 2000 to 2011, the ratio of development assistance for health for HIV to years of life saved through intervention was US$4498 in developing countries. Including in HIV-positive individuals, all-form tuberculosis incidence was 7·5 million (7·4 million to 7·7 million), prevalence was 11·9 million (11·6 million to 12·2 million), and number of deaths was 1·4 million (1·3 million to 1·5 million) in 2013. In the same year and in only individuals who were HIV-negative, all-form tuberculosis incidence was 7·1 million (6·9 million to 7·3 million), prevalence was 11·2 million (10·8 million to 11·6 million), and number of deaths was 1·3 million (1·2 million to 1·4 million). Annualised rates of change (ARC) for incidence, prevalence, and death became negative after 2000. Tuberculosis in HIV-negative individuals disproportionately occurs in men and boys (versus women and girls); 64·0% of cases (63·6 to 64·3) and 64·7% of deaths (60·8 to 70·3). Globally, malaria cases and deaths grew rapidly from 1990 reaching a peak of 232 million cases (143 million to 387 million) in 2003 and 1·2 million deaths (1·1 million to 1·4 million) in 2004. Since 2004, child deaths from malaria in sub-Saharan Africa have decreased by 31·5% (15·7 to 44·1). Outside of Africa, malaria mortality has been steadily decreasing since 1990.
Interpretation: Our estimates of the number of people living with HIV are 18·7% smaller than UNAIDS's estimates in 2012. The number of people living with malaria is larger than estimated by WHO. The number of people living with HIV, tuberculosis, or malaria have all decreased since 2000. At the global level, upward trends for malaria and HIV deaths have been reversed and declines in tuberculosis deaths have accelerated. 101 countries (74 of which are developing) still have increasing HIV incidence. Substantial progress since the Millennium Declaration is an encouraging sign of the effect of global action.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Time for a revolution in reporting of global health data.Lancet. 2014 Sep 13;384(9947):937-8. doi: 10.1016/S0140-6736(14)61062-X. Epub 2014 Jul 22. Lancet. 2014. PMID: 25059946 No abstract available.
-
MDG 6 and beyond: from halting and reversing AIDS to ending the epidemic.Lancet. 2014 Sep 13;384(9947):935-6. doi: 10.1016/S0140-6736(14)61222-8. Epub 2014 Jul 26. Lancet. 2014. PMID: 25073423 No abstract available.
-
GBD 2013 and HIV incidence in high income countries.Lancet. 2015 Mar 28;385(9974):1177. doi: 10.1016/S0140-6736(15)60626-2. Lancet. 2015. PMID: 25845784 No abstract available.
-
HIV incidence and mortality in China.Lancet. 2015 Apr 18;385(9977):1510. doi: 10.1016/S0140-6736(15)60753-X. Lancet. 2015. PMID: 25933281 No abstract available.
-
A 'needle in a haystack': Drug-induced thrombotic thrombocytopenic purpura-Association or causality?Br J Haematol. 2023 May;201(4):599-601. doi: 10.1111/bjh.18651. Epub 2023 Jan 20. Br J Haematol. 2023. PMID: 36661238
References
-
- Institute for Health Metrics and Evaluation . Financing Global Health 2013: Transition in an Age of Austerity. IHME; Seattle, WA: 2013.
-
- Floyd K, Fitzpatrick C, Pantoja A, Raviglione M. Domestic and donor financing for tuberculosis care and control in low-income and middle-income countries: an analysis of trends, 2002-11, and requirements to meet 2015 targets. Lancet Glob Health. 2013;1:e105–15. - PubMed
-
- Creese A, Floyd K, Alban A, Guinness L. Cost-effectiveness of HIV/AIDS interventions in Africa: a systematic review of the evidence. Lancet. 2002;359:1635–43. - PubMed
-
- Vassall A, Remme M. Financing tuberculosis control: promising trends and remaining challenges. Lancet Glob Health. 2013;1:e62–63. - PubMed
-
- Hecht R, Stover J, Bollinger L, Muhib F, Case K, de Ferranti D. Financing of HIV/AIDS programme scale-up in low-income and middle-income countries, 2009-31. Lancet. 2010;376:1254–60. - PubMed
Publication types
MeSH terms
Grants and funding
- 091758/WT_/Wellcome Trust/United Kingdom
- 095066/WT_/Wellcome Trust/United Kingdom
- U19 HS021110/HS/AHRQ HHS/United States
- U01 AG018947/AG/NIA NIH HHS/United States
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- UL1 TR001086/TR/NCATS NIH HHS/United States
- DA R01 003574/DA/NIDA NIH HHS/United States
- U10 CA149950/CA/NCI NIH HHS/United States
- CDF-2013-06-012/DH_/Department of Health/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- P50 AR060772/AR/NIAMS NIH HHS/United States
- KL2TR001088/TR/NCATS NIH HHS/United States
- U34 AR062891/AR/NIAMS NIH HHS/United States
- G1100684/MRC_/Medical Research Council/United Kingdom
- 099876/WT_/Wellcome Trust/United Kingdom
- KL2 TR001088/TR/NCATS NIH HHS/United States
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
