

Heterogeneous genetic alterations in sporadic nephrotic syndrome associate with resistance to immunosuppression
- PMID: 25060053
- PMCID: PMC4279734
- DOI: 10.1681/ASN.2013111155
Heterogeneous genetic alterations in sporadic nephrotic syndrome associate with resistance to immunosuppression
Abstract
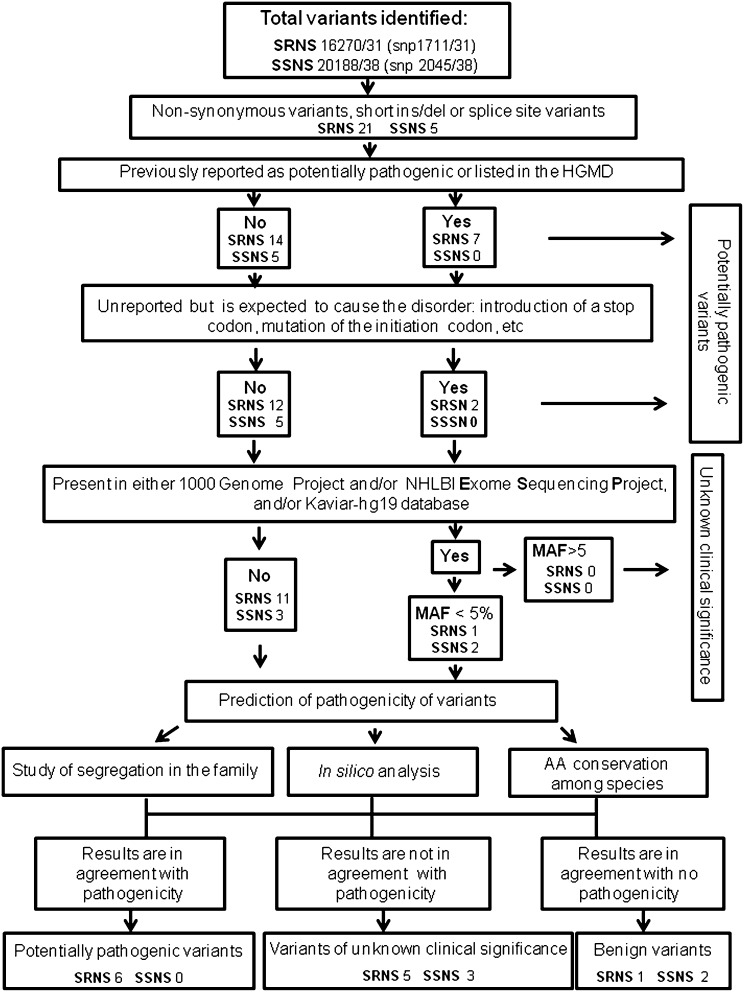
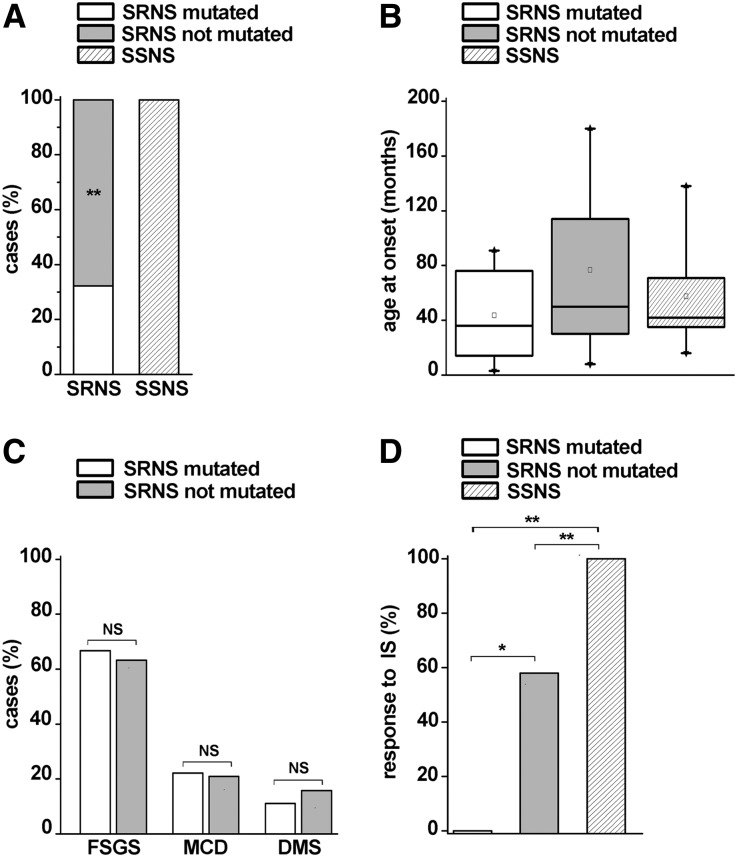
In children, sporadic nephrotic syndrome can be related to a genetic cause, but to what extent genetic alterations associate with resistance to immunosuppression is unknown. In this study, we designed a custom array for next-generation sequencing analysis of 19 target genes, reported as possible causes of nephrotic syndrome, in a cohort of 31 children affected by sporadic steroid-resistant nephrotic syndrome and 38 patients who exhibited a similar but steroid-sensitive clinical phenotype. Patients who exhibited extrarenal symptoms, had a familial history of the disease or consanguinity, or had a congenital onset were excluded. We identified a genetic cause in 32.3% of the children with steroid-resistant disease but zero of 38 children with steroid-sensitive disease. Genetic alterations also associated with lack of response to immunosuppressive agents in children with steroid-resistant disease (0% of patients with alterations versus 57.9% of patients without alterations responded to immunosuppressive agents), whereas clinical features, age at onset, and pathologic findings were similar in steroid-resistant patients with and without alterations. These results suggest that heterogeneous genetic alterations in children with sporadic forms of nephrotic syndrome associate with resistance to steroids as well as immunosuppressive treatments. In these patients, a comprehensive screening using such an array may, thus, be useful for genetic counseling and may help clinical decision making in a fast and cost-efficient manner.
Keywords: genetic variant; high-throughput DNA sequencing; immunosuppression; proteinuria.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Haraldsson B, Nyström J, Deen WM: Properties of the glomerular barrier and mechanisms of proteinuria. Physiol Rev 88: 451–487, 2008 - PubMed
-
- Wei C, Trachtman H, Li J, Dong C, Friedman AL, Gassman JJ, McMahan JL, Radeva M, Heil KM, Trautmann A, Anarat A, Emre S, Ghiggeri GM, Ozaltin F, Haffner D, Gipson DS, Kaskel F, Fischer DC, Schaefer F, Reiser J, PodoNet and FSGS CT Study Consortia : Circulating suPAR in two cohorts of primary FSGS. J Am Soc Nephrol 23: 2051–2059, 2012 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
