

Management practices and major infections after cardiac surgery
- PMID: 25060372
- PMCID: PMC4222509
- DOI: 10.1016/j.jacc.2014.04.052
Management practices and major infections after cardiac surgery
Abstract
Background: Infections are the most common noncardiac complication after cardiac surgery, but their incidence across a broad range of operations, as well as the management factors that shape infection risk, remain unknown.
Objectives: This study sought to prospectively examine the frequency of post-operative infections and associated mortality, and modifiable management practices predictive of infections within 65 days from cardiac surgery.
Methods: This study enrolled 5,158 patients and analyzed independently adjudicated infections using a competing risk model (with death as the competing event).
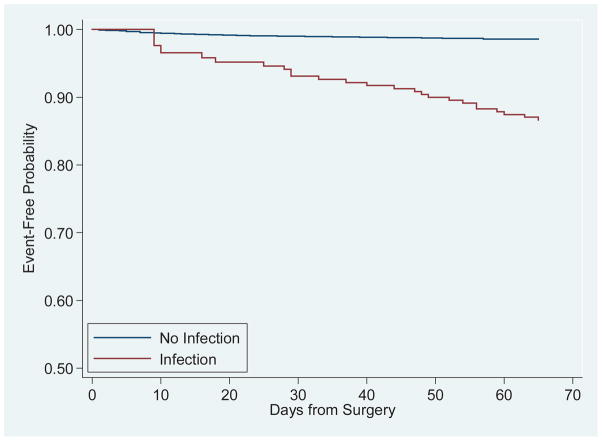
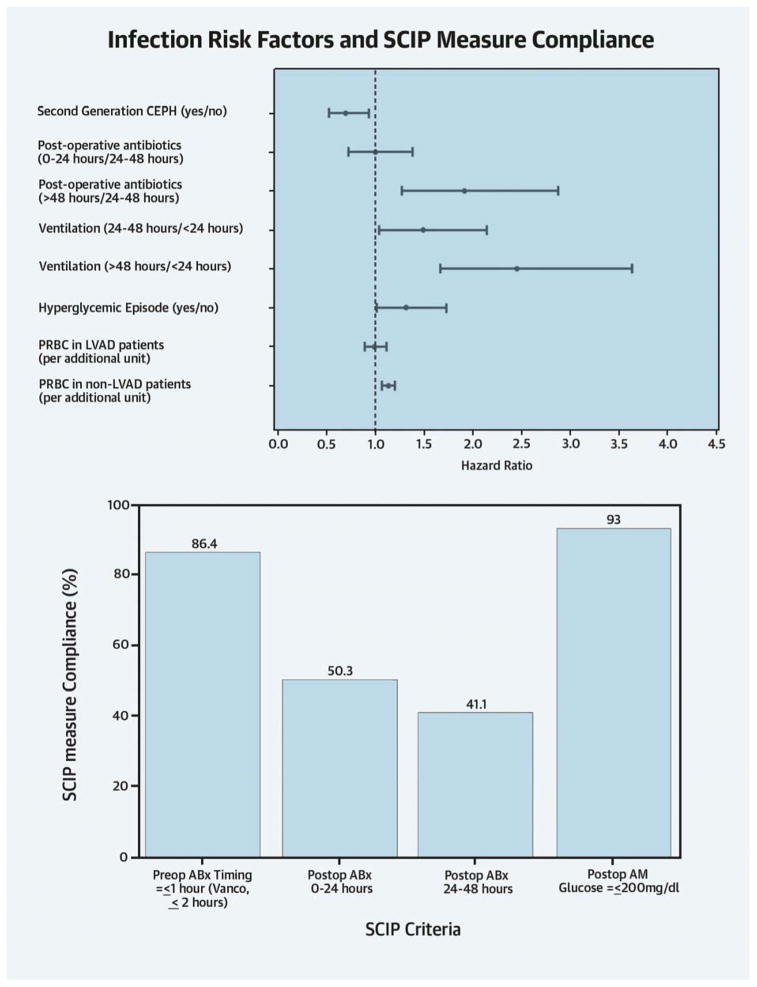
Results: Nearly 5% of patients experienced major infections. Baseline characteristics associated with increased infection risk included chronic lung disease (hazard ratio [HR]: 1.66; 95% confidence interval [CI]: 1.21 to 2.26), heart failure (HR: 1.47; 95% CI: 1.11 to 1.95), and longer surgery (HR: 1.31; 95% CI: 1.21 to 1.41). Practices associated with reduced infection risk included prophylaxis with second-generation cephalosporins (HR: 0.70; 95% CI: 0.52 to 0.94), whereas post-operative antibiotic duration >48 h (HR: 1.92; 95% CI: 1.28 to 2.88), stress hyperglycemia (HR: 1.32; 95% CI: 1.01 to 1.73); intubation time of 24 to 48 h (HR: 1.49; 95% CI: 1.04 to 2.14); and ventilation >48 h (HR: 2.45; 95% CI: 1.66 to 3.63) were associated with increased risk. HRs for infection were similar with either <24 h or <48 h of antibiotic prophylaxis. There was a significant but differential effect of transfusion by surgery type (excluding left ventricular assist device procedures/transplant) (HR: 1.13; 95% CI: 1.07 to 1.20). Major infections substantially increased mortality (HR: 10.02; 95% CI: 6.12 to 16.39).
Conclusions: Major infections dramatically affect survival and readmissions. Second-generation cephalosporins were strongly associated with reduced major infection risk, but optimal duration of antibiotic prophylaxis requires further study. Given practice variations, considerable opportunities exist for improving outcomes and preventing readmissions. (Management Practices and Risk of Infection Following Cardiac Surgery; NCT01089712).
Keywords: cardiac surgery; infection; risk factors.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Infections post-cardiac surgery: new information during challenging times.J Am Coll Cardiol. 2014 Jul 29;64(4):382-4. doi: 10.1016/j.jacc.2014.04.050. J Am Coll Cardiol. 2014. PMID: 25060373 No abstract available.
References
-
- Perencevich EN, Pittet D. Preventing catheter-related bloodstream infections. Thinking outside the checklist. JAMA. 2009;301:1285–7. - PubMed
-
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725–32. - PubMed
-
- Fowler VG, Jr, O’Brien SM, Muhlbaier LH, et al. Clinical predictors of major infections after cardiac surgery. Circulation. 2005;112:I358–65. - PubMed
-
- Abboud CS, Wey SB, Baltar VT. Risk factors for mediastinitis after cardiac surgery. Ann Thorac Surg. 2004;77:676–83. - PubMed
-
- Bode LG, Kluytmans JA, Wertheim HF, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362:9–17. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
