

Diabetes and cardiovascular disease in older adults: current status and future directions
- PMID: 25060886
- PMCID: PMC4113072
- DOI: 10.2337/db14-0020
Diabetes and cardiovascular disease in older adults: current status and future directions
Abstract
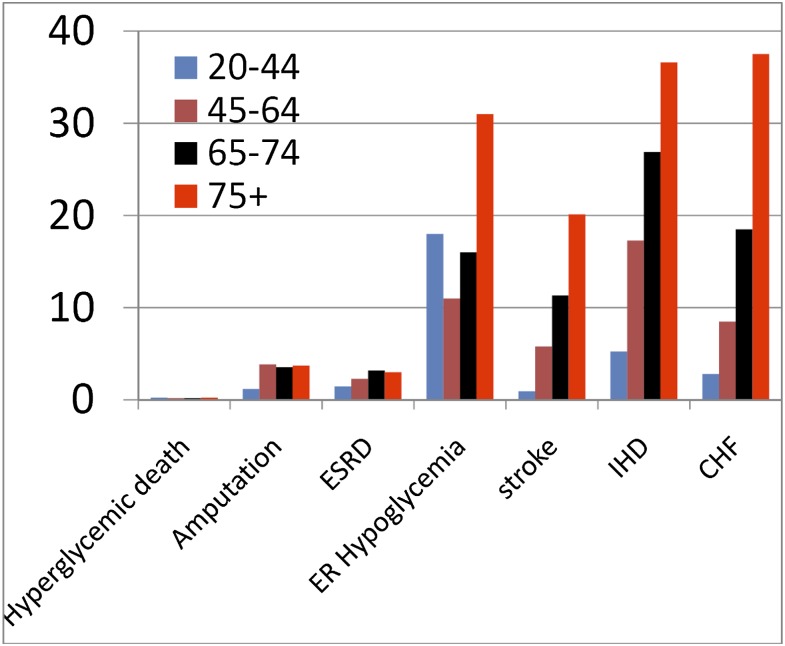
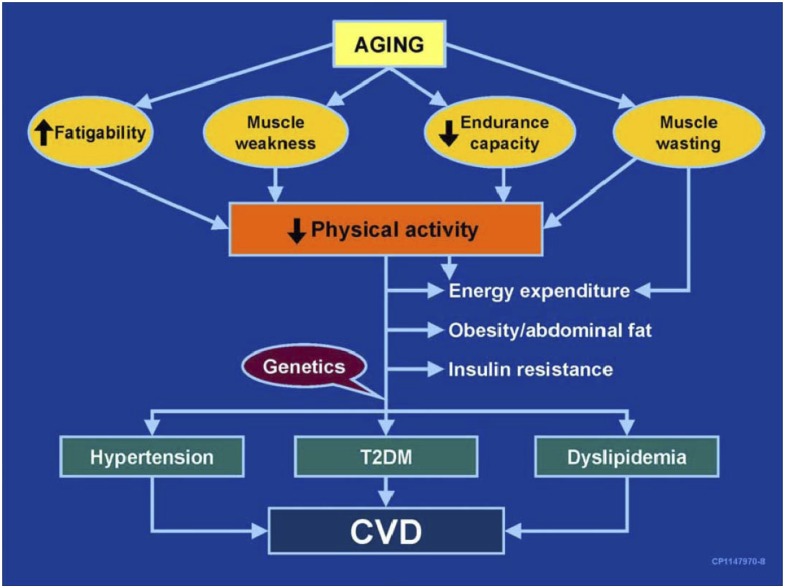
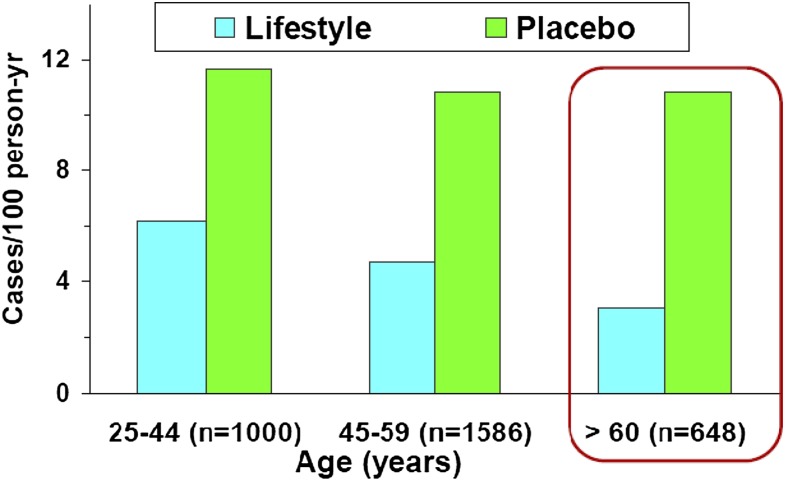
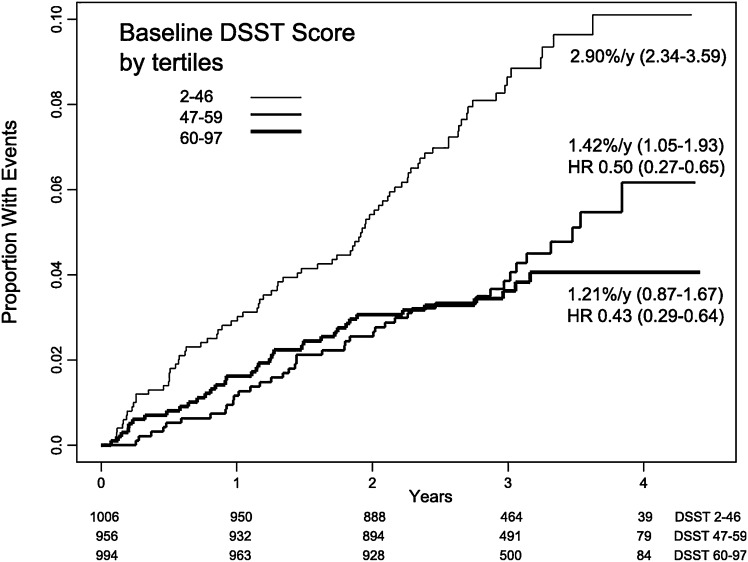
The prevalence of diabetes increases with age, driven in part by an absolute increase in incidence among adults aged 65 years and older. Individuals with diabetes are at higher risk for cardiovascular disease, and age strongly predicts cardiovascular complications. Inflammation and oxidative stress appear to play some role in the mechanisms underlying aging, diabetes, cardiovascular disease, and other complications of diabetes. However, the mechanisms underlying the age-associated increase in risk for diabetes and diabetes-related cardiovascular disease remain poorly understood. Moreover, because of the heterogeneity of the older population, a lack of understanding of the biology of aging, and inadequate study of the effects of treatments on traditional complications and geriatric conditions associated with diabetes, no consensus exists on the optimal interventions for older diabetic adults. The Association of Specialty Professors, along with the National Institute on Aging, the National Institute of Diabetes and Digestive and Kidney Diseases, the National Heart, Lung, and Blood Institute, and the American Diabetes Association, held a workshop, summarized in this Perspective, to discuss current knowledge regarding diabetes and cardiovascular disease in older adults, identify gaps, and propose questions to guide future research.
© 2014 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Centers for Disease Control and Prevention National diabetes fact sheet 2011, 2012. Available from http://www.cdc.gov/diabetes/pubs/factsheet11.htm Accessed 28 August 2013
-
- Cigolle CT, Blaum CS, Halter JB. Diabetes and cardiovascular disease prevention in older adults. Clin Geriatr Med 2009;25:607–641, vii–viii - PubMed
-
- Kuller LH, Arnold AM, Psaty BM, et al. 10-year follow-up of subclinical cardiovascular disease and risk of coronary heart disease in the Cardiovascular Health Study. Arch Intern Med 2006;166:71–78 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
