

Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies
- PMID: 25061342
- PMCID: PMC4085309
- DOI: 10.2147/PROM.S42735
Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies
Abstract
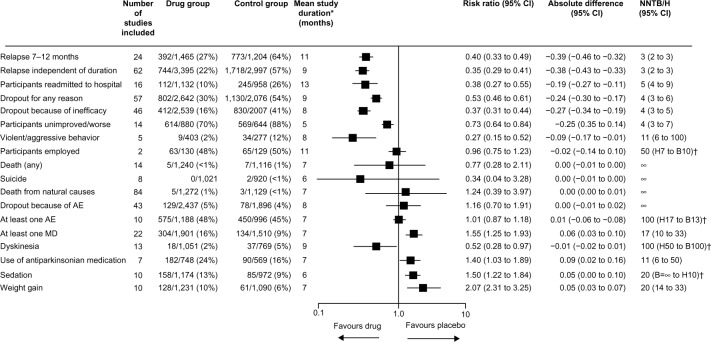
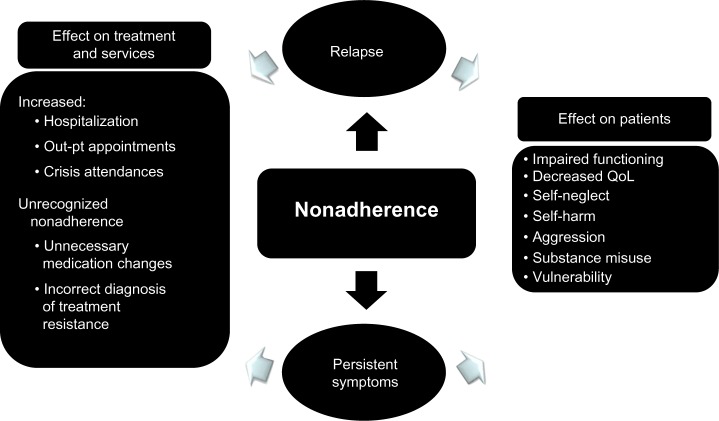
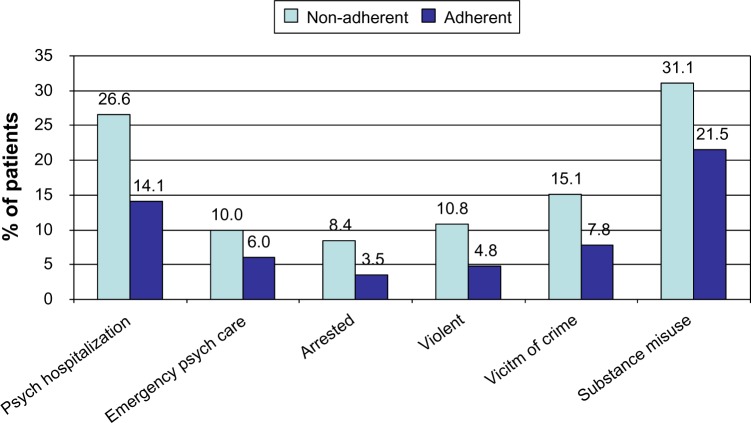
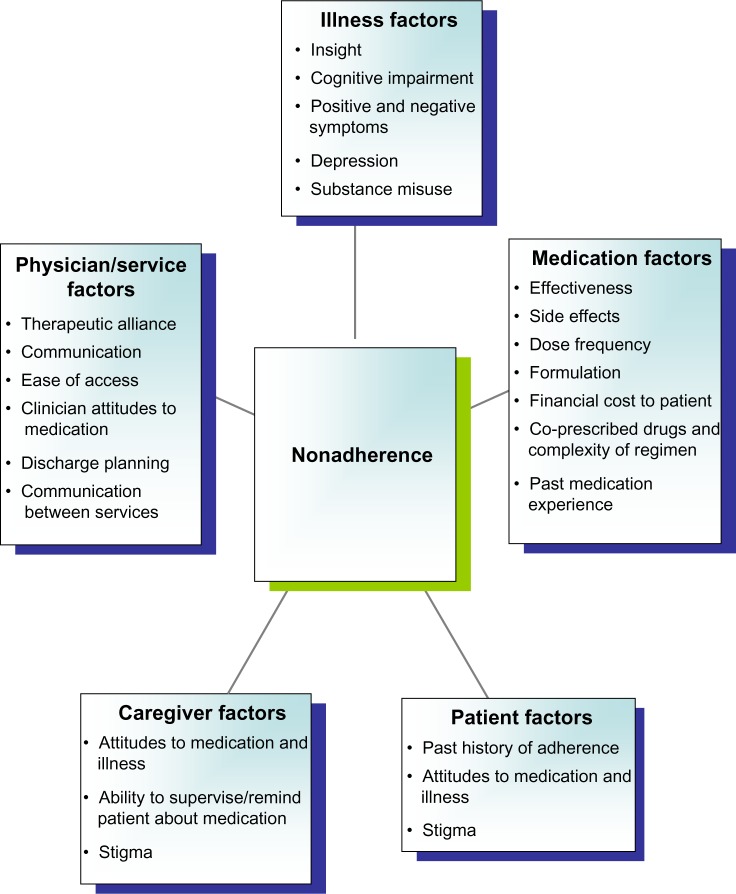
Nonadherence with medication occurs in all chronic medical disorders. It is a particular challenge in schizophrenia due to the illness's association with social isolation, stigma, and comorbid substance misuse, plus the effect of symptom domains on adherence, including positive and negative symptoms, lack of insight, depression, and cognitive impairment. Nonadherence lies on a spectrum, is often covert, and is underestimated by clinicians, but affects more than one third of patients with schizophrenia per annum. It increases the risk of relapse, rehospitalization, and self-harm, increases inpatient costs, and lowers quality of life. It results from multiple patient, clinician, illness, medication, and service factors, but a useful distinction is between intentional and unintentional nonadherence. There is no gold standard approach to the measurement of adherence as all methods have pros and cons. Interventions to improve adherence include psychoeducation and other psychosocial interventions, antipsychotic long-acting injections, electronic reminders, service-based interventions, and financial incentives. These overlap, all have some evidence of effectiveness, and the intervention adopted should be tailored to the individual. Psychosocial interventions that utilize combined approaches seem more effective than unidimensional approaches. There is increasing interest in electronic reminders and monitoring systems to enhance adherence, eg, Short Message Service text messaging and real-time medication monitoring linked to smart pill containers or an electronic ingestible event marker. Financial incentives to enhance antipsychotic adherence raise ethical issues, and their place in practice remains unclear. Simple pragmatic strategies to improve medication adherence include shared decision-making, regular assessment of adherence, simplification of the medication regimen, ensuring that treatment is effective and that side effects are managed, and promoting a positive therapeutic alliance and good communication between the clinician and patient. These elements remain essential for all patients, not least for the small minority where vulnerability and risk issue dictate that compulsory treatment is necessary to ensure adherence.
Keywords: adherence; antipsychotics; long-acting injections; nonadherence; relapse; risk factors; schizophrenia.
Figures
References
-
- Lerner BH. From careless consumptives to recalcitrant patients: the historical construction of noncompliance. Soc Sci Med. 1997;45:1423–1431. - PubMed
-
- Mohler DN, Wallin DG, Dreyfus EG. Studies in the home treatment of streptococcal disease. I. Failure of patients to take penicillin by mouth as prescribed. N Engl J Med. 1955;252:1116–1118. - PubMed
-
- National Institute for Health and Clinical Excellence Medicines adherence involving patients in decisions about prescribed medicines and supporting adherence. Jan, 2009. [Accessed March 7, 2014]. (NICE clinical guideline 76). Available from: http://www.nice.org.uk/guidance/CG76. - PubMed
-
- World Health Organization . Adherence to long-term therapies: evidence for action. Geneva, Switzerland: World Health Organization; 2003. [Accessed March 7, 2014]. Available from: http://whqlibdoc.who.int/publications/2003/9241545992.pdf.
-
- Karve S, Cleves MA, Helm M, Hudson TJ, West DS, Martin BC. Good and poor adherence: optimal cut-point for adherence measures using administrative claims data. Curr Med Res Opin. 2009;25:2303–2310. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
