

Neuroimaging after mild traumatic brain injury: review and meta-analysis
- PMID: 25061565
- PMCID: PMC4107372
- DOI: 10.1016/j.nicl.2013.12.009
Neuroimaging after mild traumatic brain injury: review and meta-analysis
Abstract
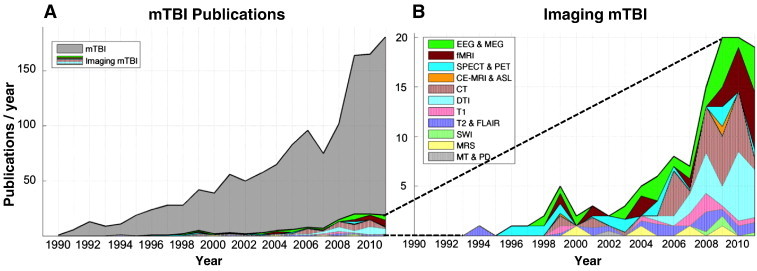
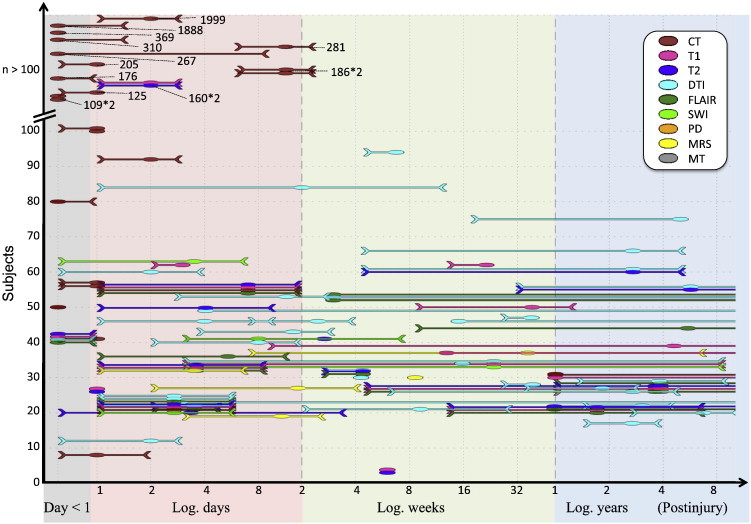
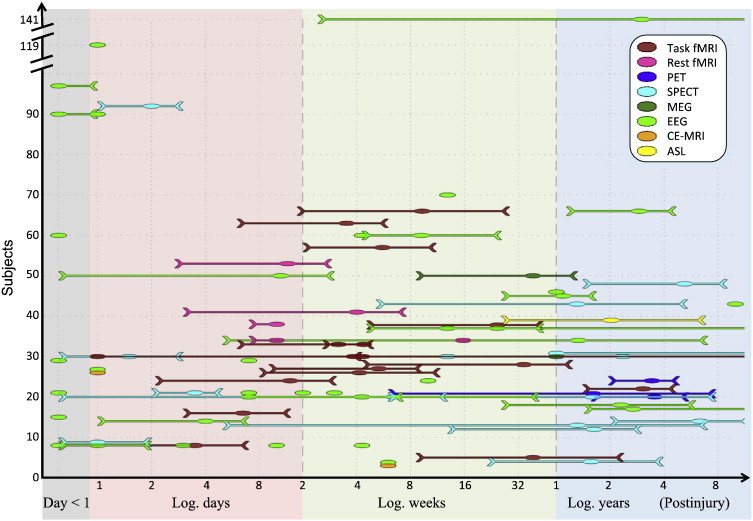
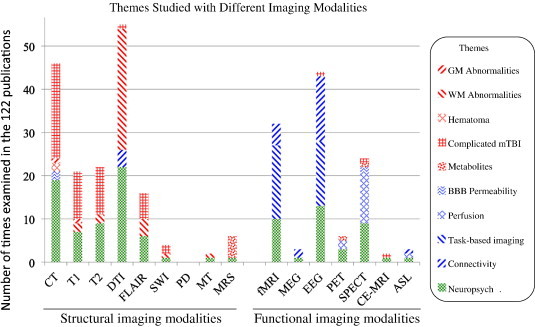
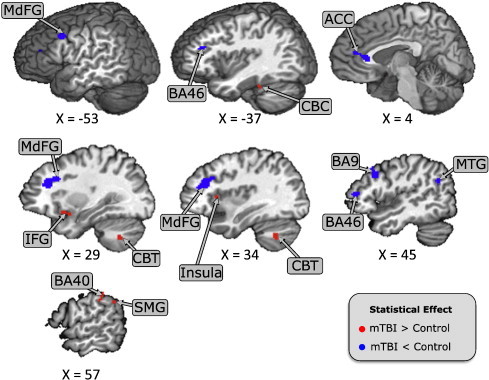
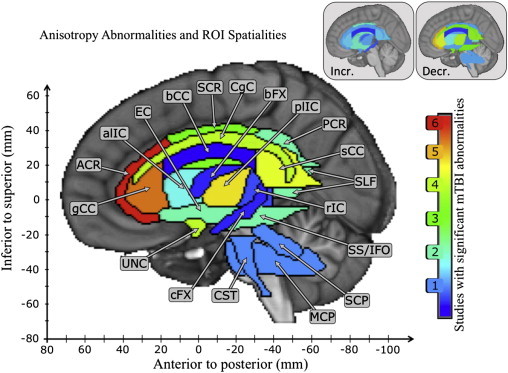
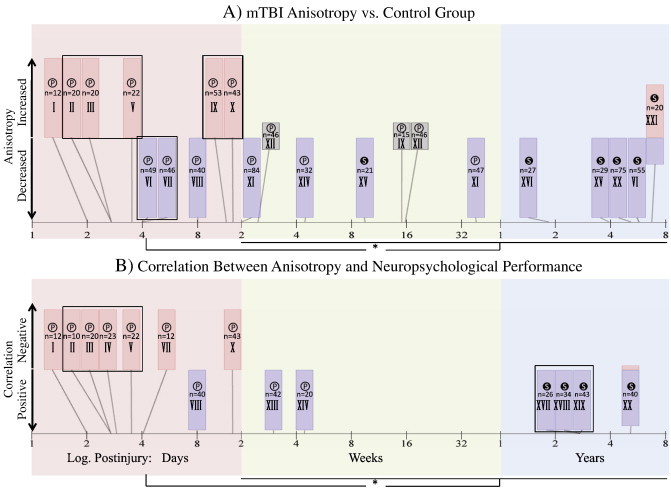
This paper broadly reviews the study of mild traumatic brain injury (mTBI), across the spectrum of neuroimaging modalities. Among the range of imaging methods, however, magnetic resonance imaging (MRI) is unique in its applicability to studying both structure and function. Thus we additionally performed meta-analyses of MRI results to examine 1) the issue of anatomical variability and consistency for functional MRI (fMRI) findings, 2) the analogous issue of anatomical consistency for white-matter findings, and 3) the importance of accounting for the time post injury in diffusion weighted imaging reports. As we discuss, the human neuroimaging literature consists of both small and large studies spanning acute to chronic time points that have examined both structural and functional changes with mTBI, using virtually every available medical imaging modality. Two key commonalities have been used across the majority of imaging studies. The first is the comparison between mTBI and control populations. The second is the attempt to link imaging results with neuropsychological assessments. Our fMRI meta-analysis demonstrates a frontal vulnerability to mTBI, demonstrated by decreased signal in prefrontal cortex compared to controls. This vulnerability is further highlighted by examining the frequency of reported mTBI white matter anisotropy, in which we show a strong anterior-to-posterior gradient (with anterior regions being more frequently reported in mTBI). Our final DTI meta-analysis examines a debated topic arising from inconsistent anisotropy findings across studies. Our results support the hypothesis that acute mTBI is associated with elevated anisotropy values and chronic mTBI complaints are correlated with depressed anisotropy. Thus, this review and set of meta-analyses demonstrate several important points about the ongoing use of neuroimaging to understand the functional and structural changes that occur throughout the time course of mTBI recovery. Based on the complexity of mTBI, however, much more work in this area is required to characterize injury mechanisms and recovery factors and to achieve clinically-relevant capabilities for diagnosis.
Keywords: DTI; Meta-analysis; Mild traumatic brain injury; Neuropsychological assessments; Post concussion syndrome; fMRI.
Figures
References
-
- Alexander M.P. Mild traumatic brain injury: pathophysiology, natural history, and clinical management. Neurology. 1995;45:1253–1260. - PubMed
-
- American Psychiatric Association . Fourth edition. American Psychiatric Association; Washington, DC: 2000. Diagnostic and Statistical Manual of Mental Disorders; pp. 760–762. (Text Revision)
-
- Bazarian J.J., Zhong J., Blyth B., Zhu T., Kavcic V. Diffusion tensor imaging detects clinically important axonal damage after mild traumatic brain injury: a pilot study. J. Neurotrauma. 2007;24:1447–1459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
