

Progression of coronary artery calcification seems to be inevitable, but predictable - results of the Heinz Nixdorf Recall (HNR) study
- PMID: 25062951
- PMCID: PMC4223611
- DOI: 10.1093/eurheartj/ehu288
Progression of coronary artery calcification seems to be inevitable, but predictable - results of the Heinz Nixdorf Recall (HNR) study
Abstract
Aim: Coronary artery calcification (CAC), as a sign of atherosclerosis, can be detected and progression quantified using computed tomography (CT). We develop a tool for predicting CAC progression.
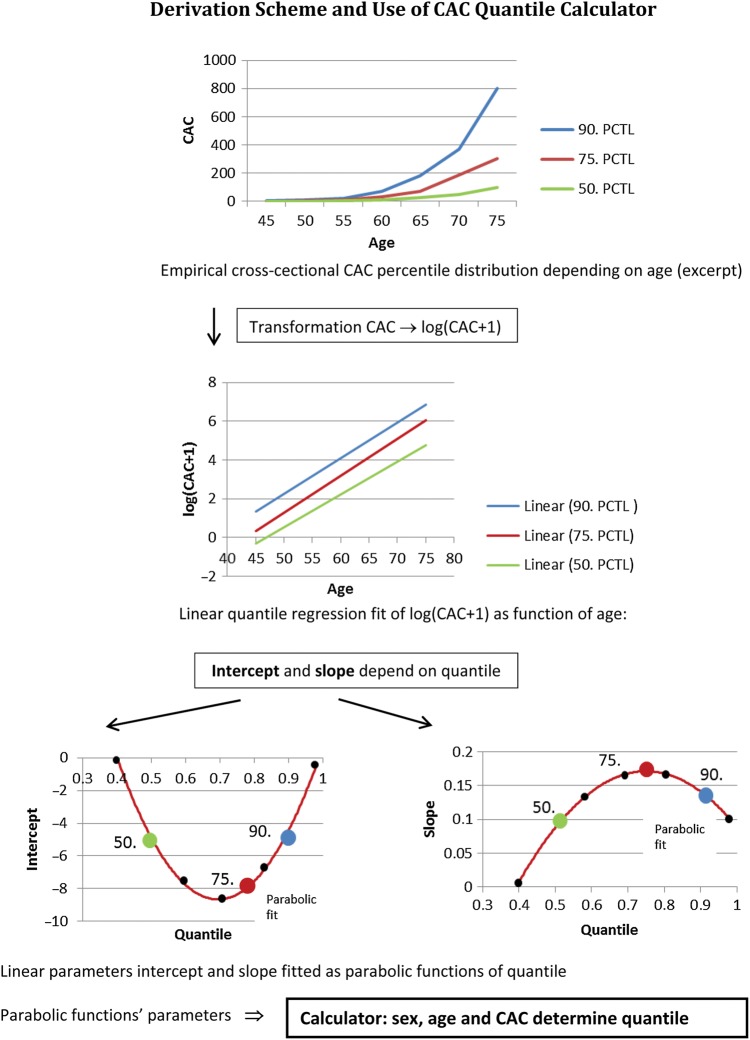
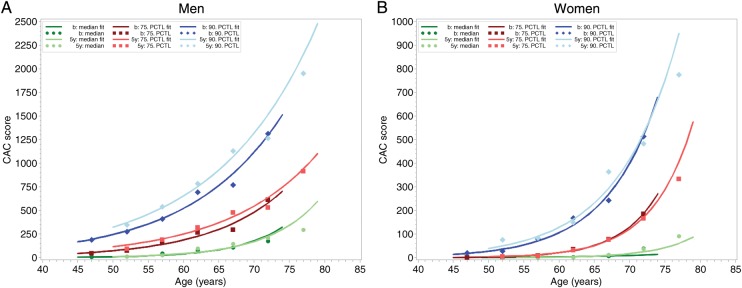
Methods and results: In 3481 participants (45-74 years, 53.1% women) CAC percentiles at baseline (CACb) and after five years (CAC₅y) were evaluated, demonstrating progression along gender-specific percentiles, which showed exponentially shaped age-dependence. Using quantile regression on the log-scale (log(CACb+1)) we developed a tool to individually predict CAC₅y, and compared to observed CAC₅y. The difference between observed and predicted CAC₅y (log-scale, mean±SD) was 0.08±1.11 and 0.06±1.29 in men and women. Agreement reached a kappa-value of 0.746 (95% confidence interval: 0.732-0.760) and concordance correlation (log-scale) of 0.886 (0.879-0.893). Explained variance of observed by predicted log(CAC₅y+1) was 80.1% and 72.0% in men and women, and 81.0 and 73.6% including baseline risk factors. Evaluating the tool in 1940 individuals with CACb>0 and CACb<400 at baseline, of whom 242 (12.5%) developed CAC₅y>400, yielded a sensitivity of 59.5%, specificity 96.1%, (+) and (-) predictive values of 68.3% and 94.3%. A pre-defined acceptance range around predicted CAC₅y contained 68.1% of observed CAC₅y; only 20% were expected by chance. Age, blood pressure, lipid-lowering medication, diabetes, and smoking contributed to progression above the acceptance range in men and, excepting age, in women.
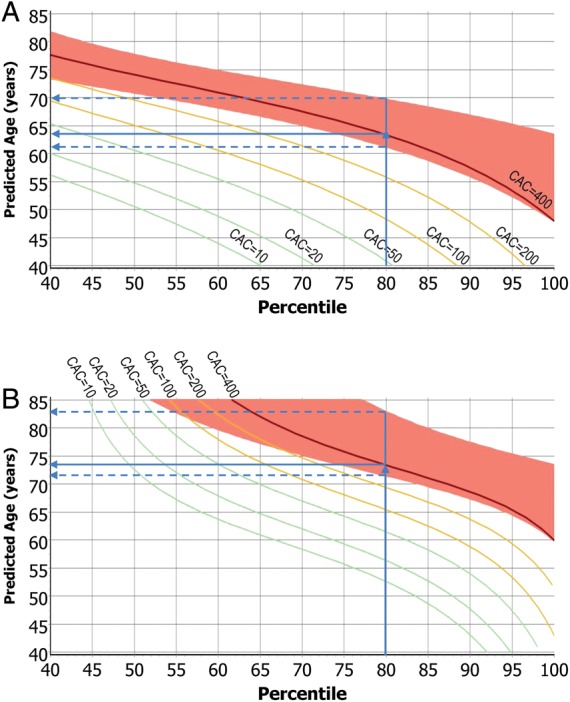
Conclusion: CAC nearly inevitably progresses with limited influence of cardiovascular risk factors. This allowed the development of a mathematical tool for prediction of individual CAC progression, enabling anticipation of the age when CAC thresholds of high risk are reached.
Keywords: CT; Coronary artery calcification; Epidemiology; Heinz Nixdorf Recall study; Imaging; Progression of atherosclerosis.
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Coronary artery disease: Predicting the progression of coronary artery calcification.Nat Rev Cardiol. 2014 Oct;11(10):557. doi: 10.1038/nrcardio.2014.117. Epub 2014 Aug 12. Nat Rev Cardiol. 2014. PMID: 25113749 No abstract available.
-
Progression of coronary calcium: not as predictable as 1-2-3.Eur Heart J. 2014 Nov 7;35(42):2934-5. doi: 10.1093/eurheartj/ehu377. Epub 2014 Sep 22. Eur Heart J. 2014. PMID: 25246484 No abstract available.
References
-
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827–832. - PubMed
-
- Min JK, Lin FY, Gidseg DS, Weinsaft JW, Weinsaft JW, Berman DS, Shaw LJ, Rozanski A, Callister TQ. Determinants of coronary calcium conversion among patients with a normal coronary calcium scan: what is the ‘warranty period’ for remaining normal? J Am Coll Cardiol. 2010;55:1110–1117. - PubMed
-
- Raggi P, Cooil B, Ratti C, Callister TQ, Budoff M. Progression of coronary artery calcium and occurrence of myocardial infarction in patients with and without diabetes mellitus. Hypertension. 2005;46:238–243. - PubMed
-
- Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, Lauer MS, Post WS, Raggi P, Redberg RF, Rodgers GP, Shaw LJ, Taylor AJ, Weintraub WS. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2007;49:378–402. - PubMed
-
- Budoff MJ, Hokanson JE, Nasir K, Shaw LJ, Kinney GL, Chow D, Demoss D, Nuguri V, Nabavi V, Ratakonda R, Berman DS, Raggi P. Progression of coronary artery calcium predicts all-cause mortality. JACC Cardiovasc Imaging. 2010;3:1229–1236. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
