

European perspective on multiple myeloma treatment strategies in 2014
- PMID: 25063227
- PMCID: PMC4122482
- DOI: 10.1634/theoncologist.2014-0042
European perspective on multiple myeloma treatment strategies in 2014
Abstract
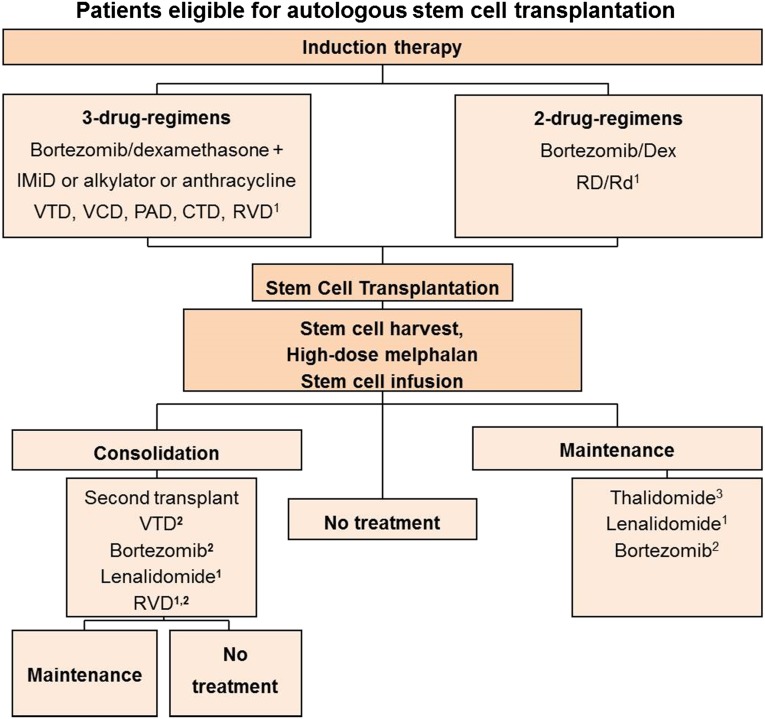
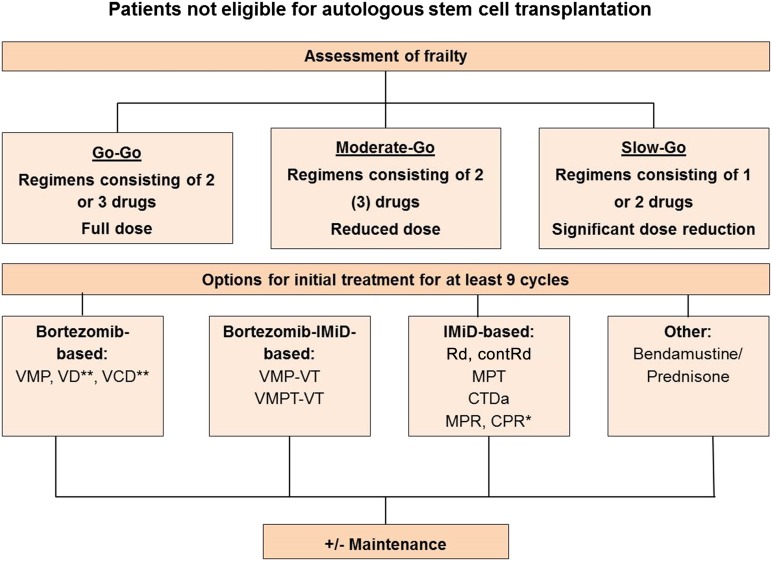
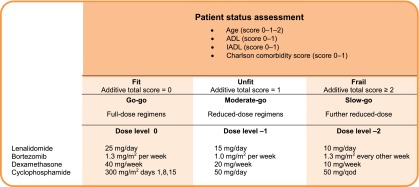
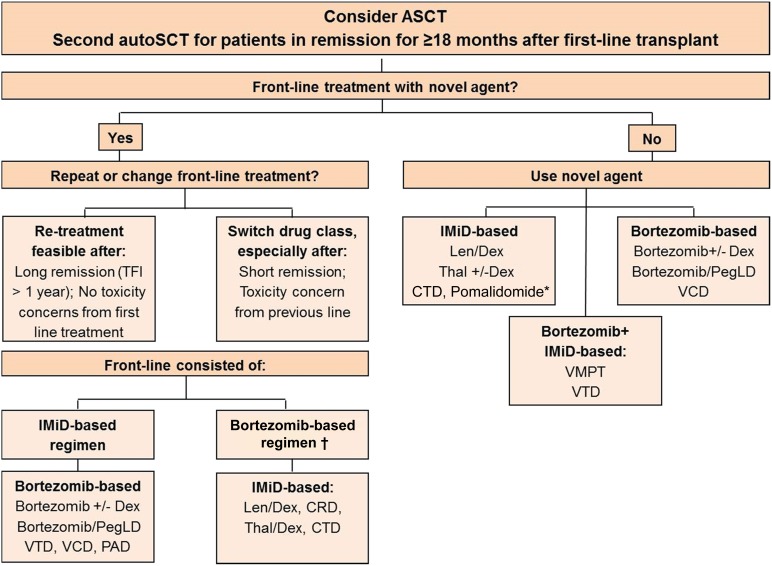
The treatment of multiple myeloma has undergone significant changes and has resulted in the achievement of molecular remissions, the prolongation of remission duration, and extended survival becoming realistic goals, with a cure being possible in a small but growing number of patients. In addition, nowadays it is possible to categorize patients more precisely into different risk groups, thus allowing the evaluation of therapies in different settings and enabling a better comparison of results across trials. Here, we review the evidence from clinical studies, which forms the basis for our recommendations for the management of patients with myeloma. Treatment approaches depend on "fitness," with chronological age still being an important discriminator for selecting therapy. In younger, fit patients, a short three drug-based induction treatment followed by autologous stem cell transplantation (ASCT) remains the preferred option. Consolidation and maintenance therapy are attractive strategies not yet approved by the European Medicines Agency, and a decision regarding post-ASCT therapy should only be made after detailed discussion of the pros and cons with the individual patient. Two- and three-drug combinations are recommended for patients not eligible for transplantation. Treatment should be administered for at least nine cycles, although different durations of initial therapy have only rarely been compared so far. Comorbidity and frailty should be thoroughly assessed in elderly patients, and treatment must be adapted to individual needs, carefully selecting appropriate drugs and doses. A substantial number of new drugs and novel drug classes in early clinical development have shown promising activity. Their introduction into clinical practice will most likely further improve treatment results.
Keywords: Autologous stem cell transplantation; Consolidation; Elderly patients; Maintenance; Multiple myeloma; Nontransplant setting; Risk stratification.
©AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Brenner H, Gondos A, Pulte D. Recent major improvement in long-term survival of younger patients with multiple myeloma. Blood. 2008;111:2521–2526. - PubMed
-
- Venner CP, Connors JM, Sutherland HJ, et al. Novel agents improve survival of transplant patients with multiple myeloma including those with high-risk disease defined by early relapse (<12 months) Leuk Lymphoma. 2011;52:34–41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
