

Vascular access choice in incident hemodialysis patients: a decision analysis
- PMID: 25063436
- PMCID: PMC4279737
- DOI: 10.1681/ASN.2013111236
Vascular access choice in incident hemodialysis patients: a decision analysis
Abstract
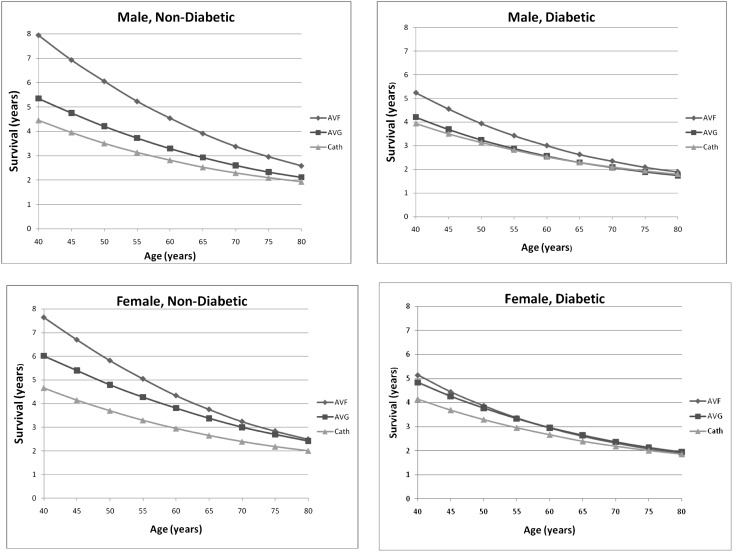
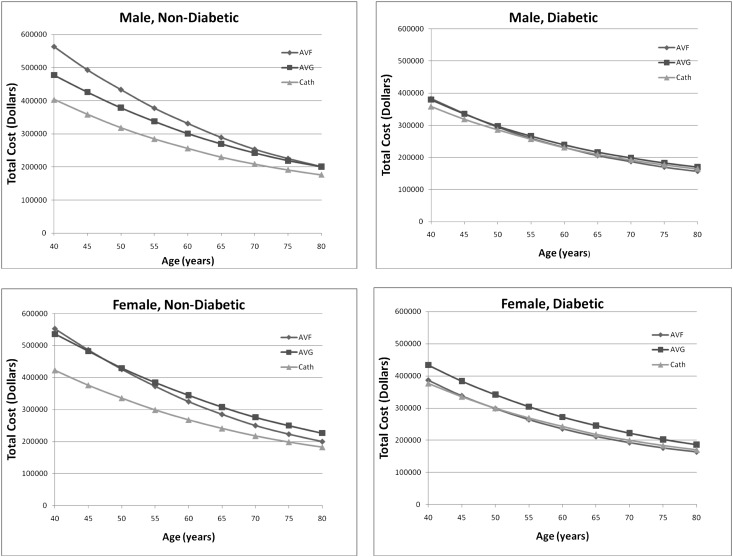
Hemodialysis vascular access recommendations promote arteriovenous (AV) fistulas first; however, it may not be the best approach for all hemodialysis patients, because likelihood of successful fistula placement, procedure-related and subsequent costs, and patient survival modify the optimal access choice. We performed a decision analysis evaluating AV fistula, AV graft, and central venous catheter (CVC) strategies for patients initiating hemodialysis with a CVC, a scenario occurring in over 70% of United States dialysis patients. A decision tree model was constructed to reflect progression from hemodialysis initiation. Patients were classified into one of three vascular access choices: maintain CVC, attempt fistula, or attempt graft. We explicitly modeled probabilities of primary and secondary patency for each access type, with success modified by age, sex, and diabetes. Access-specific mortality was incorporated using preexisting cohort data, including terms for age, sex, and diabetes. Costs were ascertained from the 2010 USRDS report and Medicare for procedure costs. An AV fistula attempt strategy was found to be superior to AV grafts and CVCs in regard to mortality and cost for the majority of patient characteristic combinations, especially younger men without diabetes. Women with diabetes and elderly men with diabetes had similar outcomes, regardless of access type. Overall, the advantages of an AV fistula attempt strategy lessened considerably among older patients, particularly women with diabetes, reflecting the effect of lower AV fistula success rates and lower life expectancy. These results suggest that vascular access-related outcomes may be optimized by considering individual patient characteristics.
Keywords: dialysis access; hemodialysis; survival.
Copyright © 2015 by the American Society of Nephrology.
Figures

Comment in
-
Catheter last, fistula not-so-first.J Am Soc Nephrol. 2015 Jan;26(1):5-7. doi: 10.1681/ASN.2014060594. Epub 2014 Jul 25. J Am Soc Nephrol. 2015. PMID: 25063435 Free PMC article. No abstract available.
References
-
- Lacson E, Jr., Wang W, Hakim RM, Teng M, Lazarus JM: Associates of mortality and hospitalization in hemodialysis: Potentially actionable laboratory variables and vascular access. Am J Kidney Dis 53: 79–90, 2009 - PubMed
-
- Pisoni RL, Arrington CJ, Albert JM, Ethier J, Kimata N, Krishnan M, Rayner HC, Saito A, Sands JJ, Saran R, Gillespie B, Wolfe RA, Port FK: Facility hemodialysis vascular access use and mortality in countries participating in DOPPS: An instrumental variable analysis. Am J Kidney Dis 53: 475–491, 2009 - PubMed
-
- Fistual First Breakthrough Initiative. Available at: http://www.fistulafirst.org/AboutFistulaFirst/FFBIData.aspx. Accessed July 7, 2013
-
- Foley RN, Chen SC, Collins AJ: Hemodialysis access at initiation in the United States, 2005 to 2007: Still “catheter first.” Hemodial Int 13: 533–542, 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
