

Understanding CBHI hospitalisation patterns: a comparison of insured and uninsured women in Gujarat, India
- PMID: 25064209
- PMCID: PMC4114097
- DOI: 10.1186/1472-6963-14-320
Understanding CBHI hospitalisation patterns: a comparison of insured and uninsured women in Gujarat, India
Abstract
Background: Community-based health insurance has been associated with increased hospitalisation in low-income settings, but with limited analysis of the illnesses for which claims are submitted. A review of claims submitted to VimoSEWA, an inpatient insurance scheme in Gujarat, India, found that fever, diarrhoea and hysterectomy, the latter at a mean age of 37 years, were the leading reasons for claims by adult women. We compared the morbidity, outpatient treatment-seeking and hospitalisation patterns of VimoSEWA-insured women with uninsured women.
Methods: We utilised data from a cross-sectional survey of 1,934 insured and uninsured women in Gujarat, India. Multivariable logistic regression identified predictors of insurance coverage and the association of insurance with hospitalisation. Self-reported data on morbidity, outpatient care and hospitalisation were compared between insured and uninsured women.
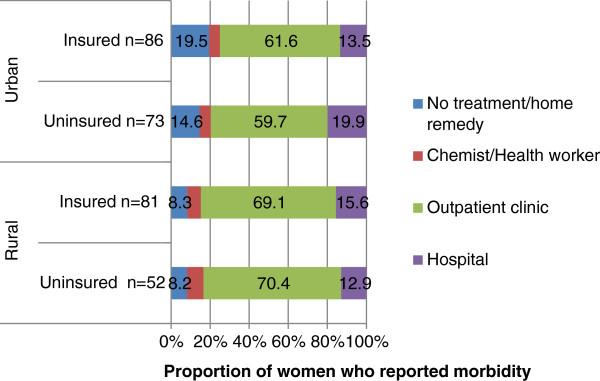
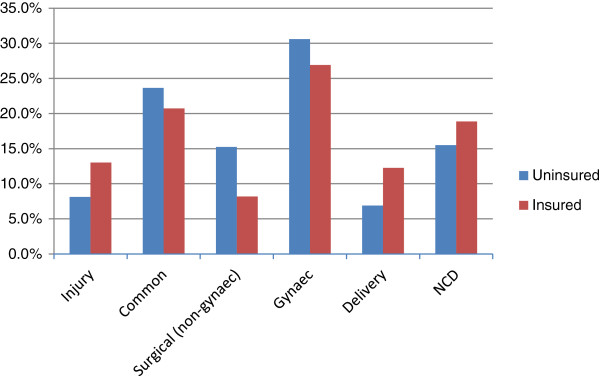
Results: Age, marital status and occupation of adult women were associated with insurance status. Reported recent morbidity, type of illness and outpatient treatment were similar among insured and uninsured women. Multivariable analysis revealed strong evidence of a higher odds of hospitalisation amongst the insured (OR = 2.7; 95% ci. 1.6, 4.7). The leading reason for hospitalisation for uninsured and insured women was hysterectomy, at a similar mean age of 36, followed by common ailments such as fever and diarrhoea. Insured women appeared to have a higher probability of being hospitalised than uninsured women for all causes, rather than specifically for fever, diarrhoea or hysterectomy. Length of stay was similar while choice of hospital differed between insured and uninsured women.
Conclusions: Despite similar reported morbidity patterns and initial treatment-seeking behaviour, VimoSEWA members were more likely to be hospitalised. The data did not provide strong evidence that inpatient hospitalisation replaced outpatient treatment for common illnesses or that insurance was the primary inducement for hysterectomy in the population. Rather, it appears that VimoSEWA members behaved differently in deciding if, and where, to be hospitalised for any condition. Further research is required to explore this decision-making process and roles, if any, played by adverse selection and moral hazard. Lastly, these hospitalisation patterns raise concerns regarding population health needs and access to quality preventive and outpatient services.
Figures
Similar articles
-
The effect of community health worker-led education on women's health and treatment-seeking: A cluster randomised trial and nested process evaluation in Gujarat, India.J Glob Health. 2017 Dec;7(2):020404. doi: 10.7189/jogh.07.020404. J Glob Health. 2017. PMID: 28959438 Free PMC article. Clinical Trial.
-
Hospitalized for fever? Understanding hospitalization for common illnesses among insured women in a low-income setting.Health Policy Plan. 2014 Jul;29(4):475-82. doi: 10.1093/heapol/czt032. Health Policy Plan. 2014. PMID: 23749652
-
Children's receipt of health care services and family health insurance patterns.Ann Fam Med. 2009 Sep-Oct;7(5):406-13. doi: 10.1370/afm.1040. Ann Fam Med. 2009. PMID: 19752468 Free PMC article.
-
Caesarean section in uninsured women in the USA: systematic review and meta-analysis.BMJ Open. 2019 Mar 3;9(3):e025356. doi: 10.1136/bmjopen-2018-025356. BMJ Open. 2019. PMID: 30833323 Free PMC article.
-
[(No) Treatment for people without health insurance coverage : When access to inpatient surgical care is denied].Chirurgie (Heidelb). 2025 Mar;96(3):205-212. doi: 10.1007/s00104-024-02234-3. Epub 2025 Feb 3. Chirurgie (Heidelb). 2025. PMID: 39900750 Review. German.
Cited by
-
Predictors of hysterectomy among married women 15-49 years in India.Reprod Health. 2018 Jan 5;15(1):3. doi: 10.1186/s12978-017-0445-8. Reprod Health. 2018. PMID: 29304867 Free PMC article.
-
Exploring Factors Influencing Family's Enrollment in Community-Based Health Insurance in the City of Gondar Peri-Urban Community, Northwest Ethiopia: A Health Belief Model Approach.Risk Manag Healthc Policy. 2024 Mar 15;17:603-622. doi: 10.2147/RMHP.S454683. eCollection 2024. Risk Manag Healthc Policy. 2024. PMID: 38510339 Free PMC article.
-
Incidence and determinants of hysterectomy in a low-income setting in Gujarat, India.Health Policy Plan. 2017 Feb;32(1):68-78. doi: 10.1093/heapol/czw099. Epub 2016 Aug 6. Health Policy Plan. 2017. PMID: 27497139 Free PMC article.
References
-
- Soors W, Devadasan N, Durairaj V, Criel B. World Health Report Background Report. Vol. 14. Geneva: WHO; 2010. Community Health Insurance and Universal Coverage: Multiple paths, many rivers to cross.
-
- Radermacher R, Ashok S, Zabel K, Dror I. What do we know about the impact of microinsurance? New Delhi, India: Microinsurance Academy; 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
