

Empirical evidence for discrete neurocognitive subgroups in bipolar disorder: clinical implications
- PMID: 25065409
- PMCID: PMC4797987
- DOI: 10.1017/S0033291714000439
Empirical evidence for discrete neurocognitive subgroups in bipolar disorder: clinical implications
Abstract
Background: Recent data suggest trait-like neurocognitive impairments in bipolar disorder (BPD), with deficits about 1 s.d. below average, less severe than deficits noted in schizophrenia. The frequency of significant impairment in BPD is approximately 60%, with 40% of patients characterized as cognitively spared. This contrasts with a more homogeneous presentation in schizophrenia. It is not understood why some BPD patients develop deficits while others do not.
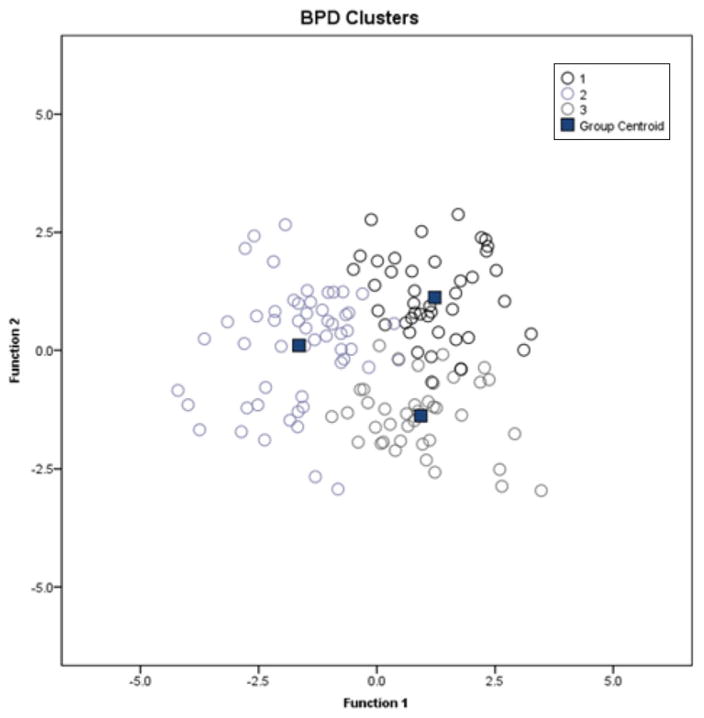
Method: A total of 136 patients with BPD completed the MATRICS Consensus Cognitive Battery and data were entered into hierarchical cluster analyses to: (1) determine the optimal number of clusters (subgroups) that fit the sample; and (2) assign subjects to a specific cluster based on individual profiles. We then compared subgroups on several clinical factors and real-world community functioning.
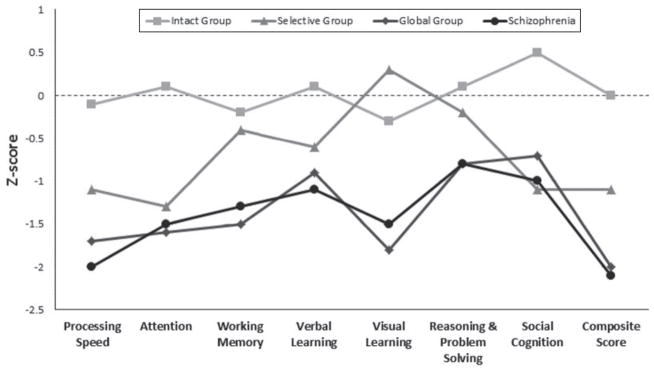
Results: Three distinct neurocognitive subgroups were found: (1) an intact group with performance comparable with healthy controls on all domains but with superior social cognition; (2) a selective impairment group with moderate deficits on processing speed, attention, verbal learning and social cognition and normal functioning in other domains; and (3) a global impairment group with severe deficits across all cognitive domains comparable with deficits in schizophrenia.
Conclusions: These results suggest the presence of multiple cognitive subgroups in BPD with unique profiles and begin to address the relationships between these subgroups, several clinical factors and functional outcome. Next steps will include using these data to help guide future efforts to target these disabling symptoms with treatment.
Conflict of interest statement
K.E.B. has served on an advisory board for Dainippon Sumitomo Pharma. A.K.M. has served as consultant or speaker for Bristol-Myers Squibb, Merck, AstraZeneca, Vanda Pharmaceuticals and Clinical Data Inc., and has received research support from Pfizer, Janssen Pharmaceuticals, Bristol-Myers Squibb and Eli Lilly. S.F. serves on advisory boards for Enzymotec and Janssen-Cilag.
Figures
Comment in
-
Letter to the Editor: Neuropsychological subgroups are evident in both mood and psychosis spectrum disorders.Psychol Med. 2014 Jul;44(9):2015. doi: 10.1017/S0033291714001019. Psychol Med. 2014. PMID: 25266118 No abstract available.
References
-
- Abood Z, Sharkey A, Webb M, Kelly A, Gill M. Are patients with bipolar affective disorder socially disadvantaged? A comparison with a control group. Bipolar Disorder. 2002;4:243–248. - PubMed
-
- Altman EG, Hedeker DR, Janicak PG, Peterson JL, Davis JM. The Clinician-Administered Rating Scale for Mania (CARS-M): development, reliability, and validity. Biological Psychiatry. 1994;36:124–134. - PubMed
-
- Altshuler LL, Ventura J, van Gorp WG, Green MF, Theberge DC, Mintz J. Neurocognitive function in clinically stable men with bipolar I disorder or schizophrenia and normal control subjects. Biological Psychiatry. 2004;56:560–569. - PubMed
-
- APA. Diagnostic and Statistical Manual of Mental Disorders. 4. American Psychiatric Association; Washington, DC: 2000. DSM-IV-TR.
-
- Bora E, Yucel M, Pantelis C. Cognitive endophenotypes of bipolar disorder: a meta-analysis of neuropsychological deficits in euthymic patients and their first-degree relatives. Journal of Affective Disorders. 2009;113:1–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
