

Expected population impacts of discontinued prostate-specific antigen screening
- PMID: 25065910
- PMCID: PMC4221407
- DOI: 10.1002/cncr.28932
Expected population impacts of discontinued prostate-specific antigen screening
Abstract
Background: Prostate-specific antigen (PSA) screening for prostate cancer has high risks of overdiagnosis, particularly among older men, and reports from screening trials indicate that it saves few lives after 11 to 13 years of follow-up. New clinical guidelines recommend against PSA screening for all men or for men aged >70 years, but, to the authors' knowledge, the expected population effects of these guidelines have not been studied to date.
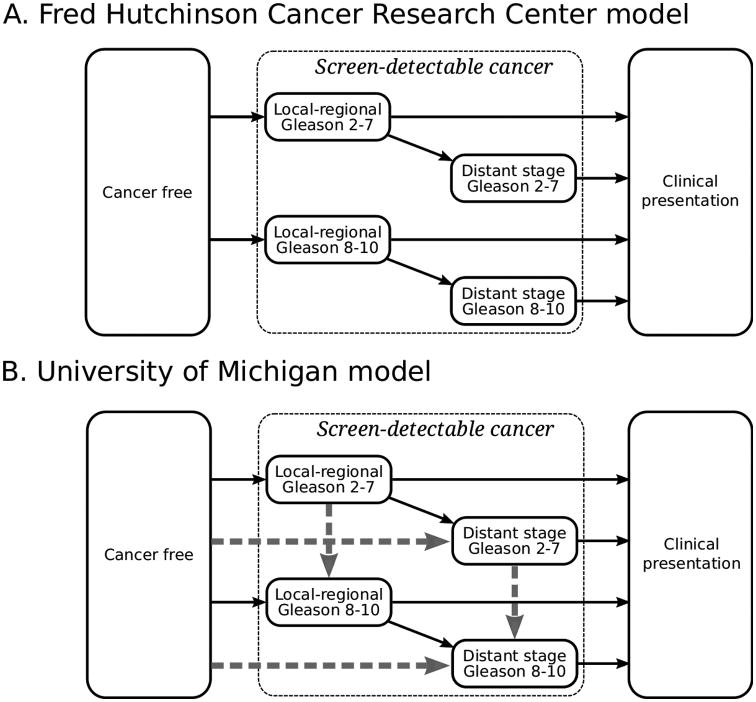
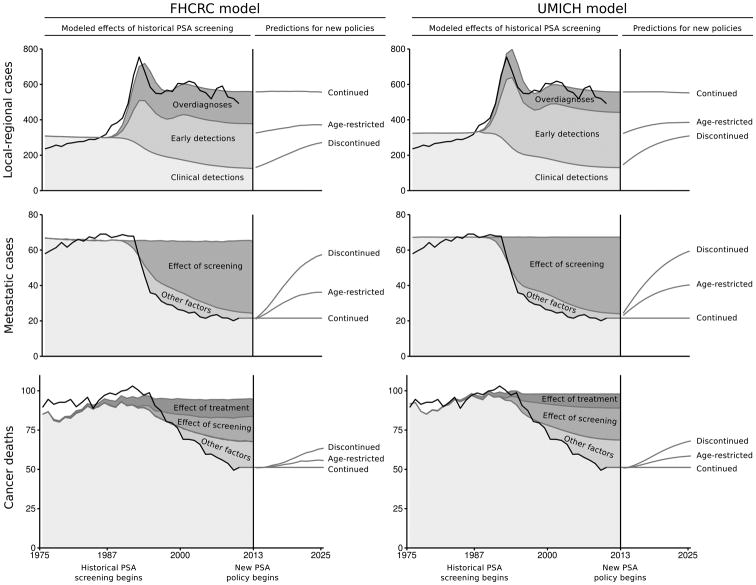
Methods: Two models of prostate cancer natural history and diagnosis were previously developed using reconstructed PSA screening patterns and prostate cancer incidence in the United States. Assuming a survival benefit of PSA screening consistent with the screening trials, the authors used the models to predict incidence and mortality rates for the period from 2013 through 2025 under continued PSA screening and under discontinued PSA screening for all men or for men aged >70 years.
Results: The models predicted that continuation of recent screening rates will overdiagnose 710,000 to 1,120,000 men (range between models) but will avoid 36,000 to 57,000 cancer deaths over the period 2013 through 2025. Discontinued screening for all men eliminated 100% of overdiagnoses but failed to prevent 100% of avoidable cancer deaths. Continued screening for men aged <70 years eliminated 64% to 66% of overdiagnoses but failed to prevent 36% to 39% of avoidable cancer deaths.
Conclusions: Discontinuing PSA screening for all men may generate many avoidable cancer deaths. Continuing PSA screening for men aged <70 years could prevent greater than one-half of these avoidable cancer deaths while dramatically reducing overdiagnoses compared with continued PSA screening for all ages.
Keywords: mass screening; models; prostate-specific antigen; prostatic neoplasms; statistical; surveillance.
© 2014 American Cancer Society.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014 Jan;64(1):9–29. - PubMed
-
- Etzioni R, Cha R, Feuer EJ, Davidov O. Asymptomatic incidence and duration of prostate cancer. Am J Epidemiol. 1998;148(8):775–785. - PubMed
-
- Etzioni R, Gulati R, Falcon S, Penson D. Impact of PSA screening on the incidence of advanced stage prostate cancer in the US: A surveillance modeling approach. Med Decis Making. 2008;28:323–331. - PubMed
-
-
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Mortality - All COD, Aggregated with State, Total U.S. (1969-2010) <Katrina/Rita Population Adjustment>, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013. Underlying mortality data provided by NCHS (www.cdc.gov/nchs).
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
