

Cost minimization using an artificial neural network sleep apnea prediction tool for sleep studies
- PMID: 25068704
- PMCID: PMC4214056
- DOI: 10.1513/AnnalsATS.201404-161OC
Cost minimization using an artificial neural network sleep apnea prediction tool for sleep studies
Abstract
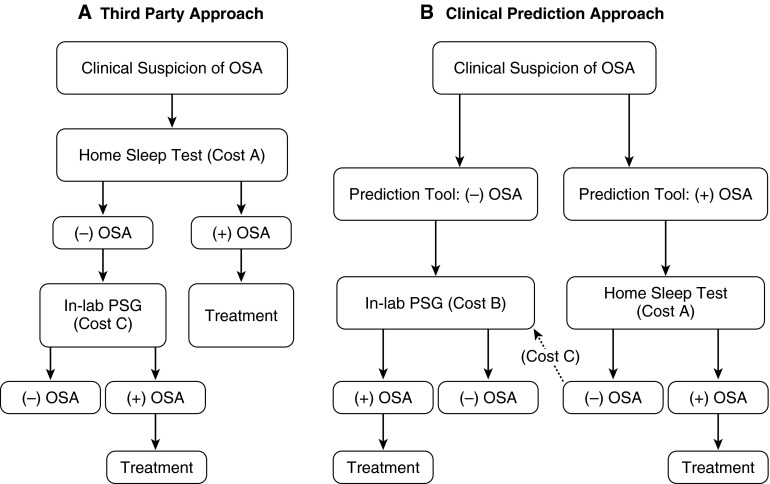
Rationale: More than a million polysomnograms (PSGs) are performed annually in the United States to diagnose obstructive sleep apnea (OSA). Third-party payers now advocate a home sleep test (HST), rather than an in-laboratory PSG, as the diagnostic study for OSA regardless of clinical probability, but the economic benefit of this approach is not known.
Objectives: We determined the diagnostic performance of OSA prediction tools including the newly developed OSUNet, based on an artificial neural network, and performed a cost-minimization analysis when the prediction tools are used to identify patients who should undergo HST.
Methods: The OSUNet was trained to predict the presence of OSA in a derivation group of patients who underwent an in-laboratory PSG (n = 383). Validation group 1 consisted of in-laboratory PSG patients (n = 149). The network was trained further in 33 patients who underwent HST and then was validated in a separate group of 100 HST patients (validation group 2). Likelihood ratios (LRs) were compared with two previously published prediction tools. The total costs from the use of the three prediction tools and the third-party approach within a clinical algorithm were compared.
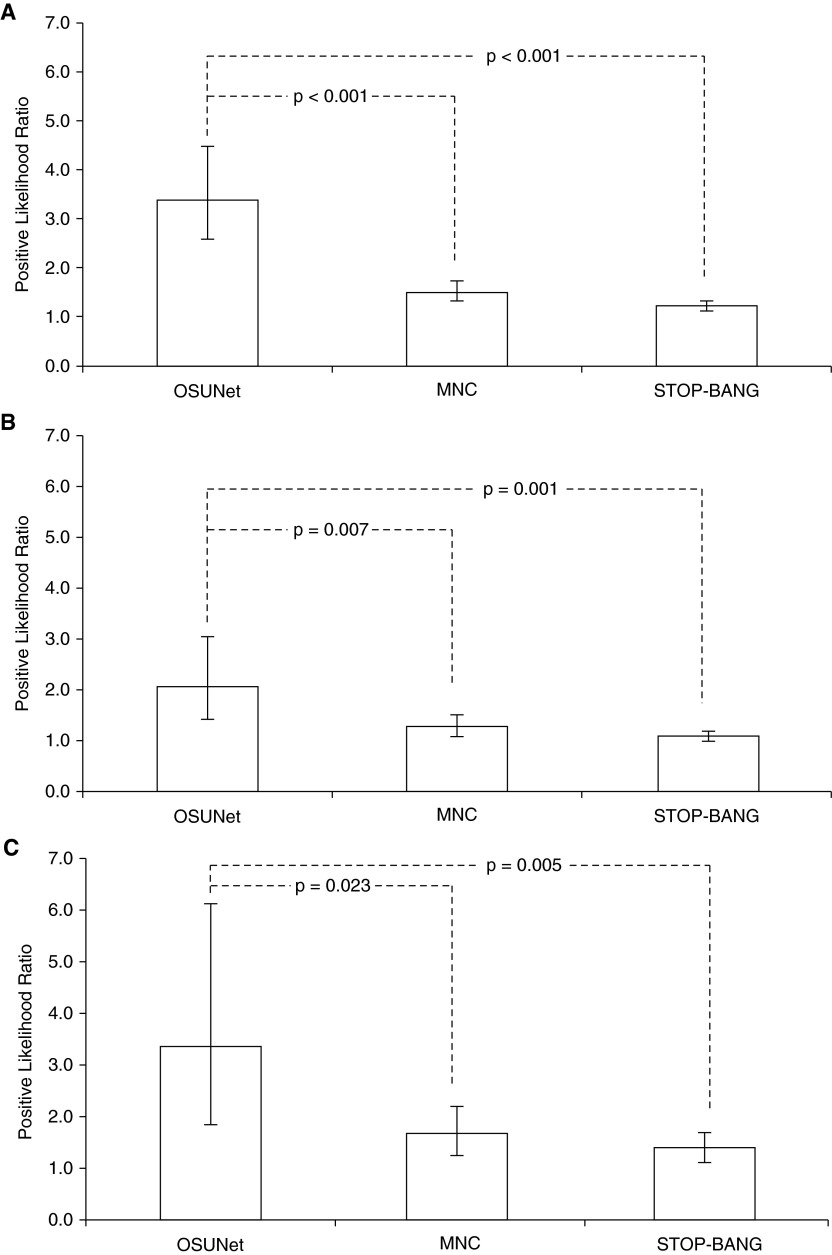
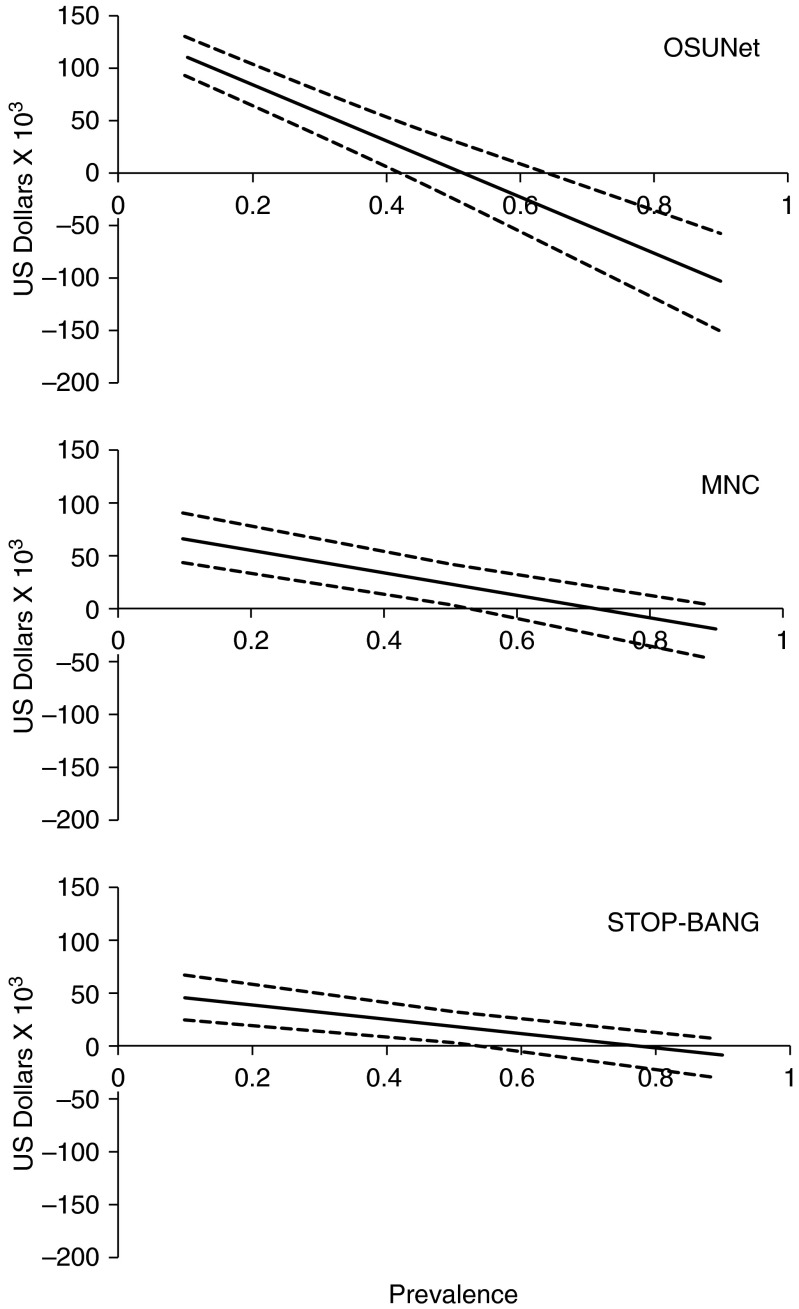
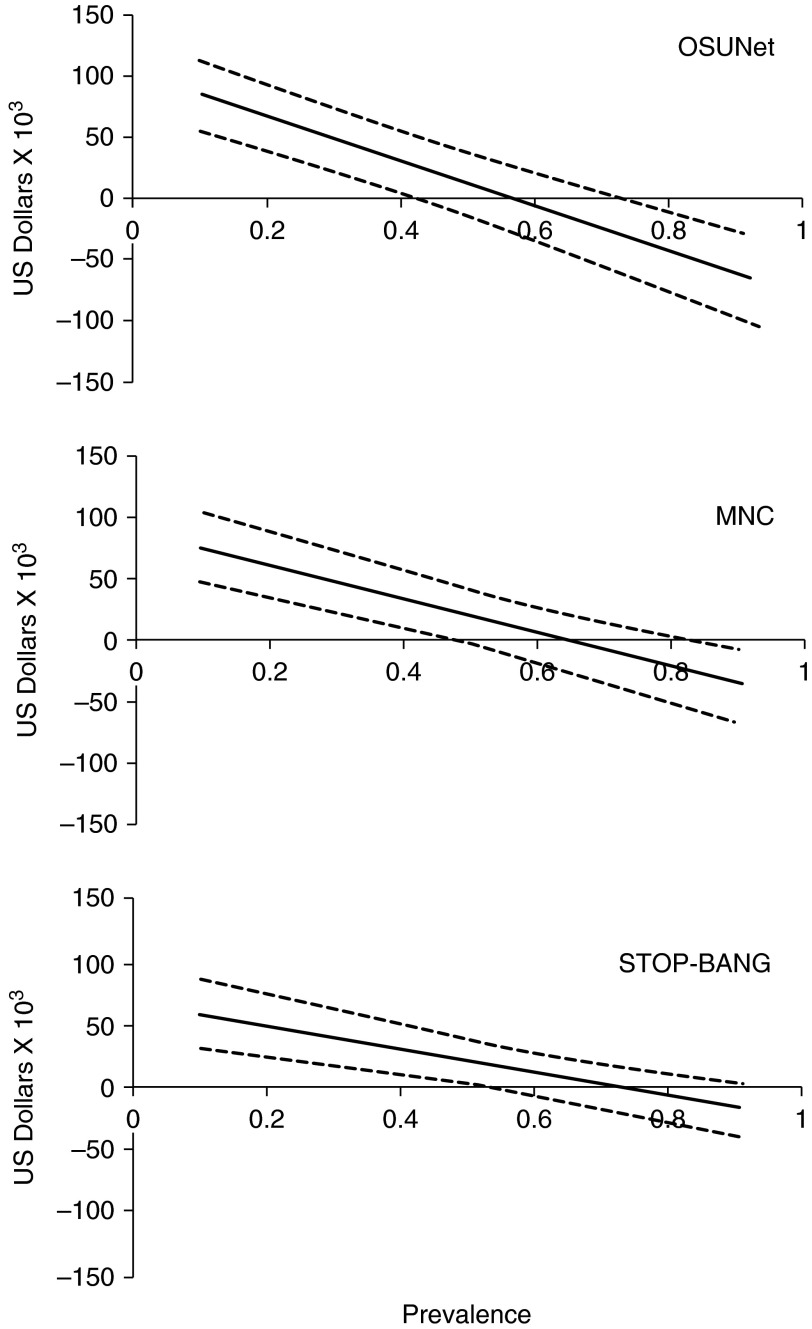
Measurements and main results: The OSUNet had a higher +LR in all groups compared with the STOP-BANG and the modified neck circumference (MNC) prediction tools. The +LRs for STOP-BANG, MNC, and OSUNet in validation group 1 were 1.1 (1.0-1.2), 1.3 (1.1-1.5), and 2.1 (1.4-3.1); and in validation group 2 they were 1.4 (1.1-1.7), 1.7 (1.3-2.2), and 3.4 (1.8-6.1), respectively. With an OSA prevalence less than 52%, the use of all three clinical prediction tools resulted in cost savings compared with the third-party approach.
Conclusions: The routine requirement of an HST to diagnose OSA regardless of clinical probability is more costly compared with the use of OSA clinical prediction tools that identify patients who should undergo this procedure when OSA is expected to be present in less than half of the population. With OSA prevalence less than 40%, the OSUNet offers the greatest savings, which are substantial when the number of sleep studies done annually is considered.
Keywords: clinical prediction rule; cost analysis; neural network models; sleep-disordered breathing.
Figures
References
-
- Tachibana N, Ayas NT, White DP. A quantitative assessment of sleep laboratory activity in the United States. J Clin Sleep Med. 2005;1:23–26. - PubMed
-
- Ayas NT, Fox J, Epstein L, Ryan CF, Fleetham JA. Initial use of portable monitoring versus polysomnography to confirm obstructive sleep apnea in symptomatic patients: an economic decision model. Sleep Med. 2010;11:320–324. - PubMed
-
- Collop NA, Anderson WM, Boehlecke B, Claman D, Goldberg R, Gottlieb DJ, Hudgel D, Sateia M, Schwab R Portable Monitoring Task Force of the American Academy of Sleep Medicine. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. J Clin Sleep Med. 2007;3:737–747. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
