

Treatment patterns and outcomes for patients with adrenocortical carcinoma associated with hospital case volume in the United States
- PMID: 25069860
- PMCID: PMC4515350
- DOI: 10.1245/s10434-014-3931-z
Treatment patterns and outcomes for patients with adrenocortical carcinoma associated with hospital case volume in the United States
Abstract
Background: Adrenocortical carcinoma (ACC) is a rare, aggressive disease with no apparent change in treatment or survival in the United States over the past two decades. Our objective was to determine whether treatment patterns or clinical outcomes vary by hospital case volume.
Methods: Patients with ACC were identified from the National Cancer Database (1998-2011). High-volume centers (HVCs) were defined by a case load of ≥4 cases of primary adrenal malignancy annually, which corresponded to the 90th percentile. All other facilities were considered low-volume centers (LVCs).
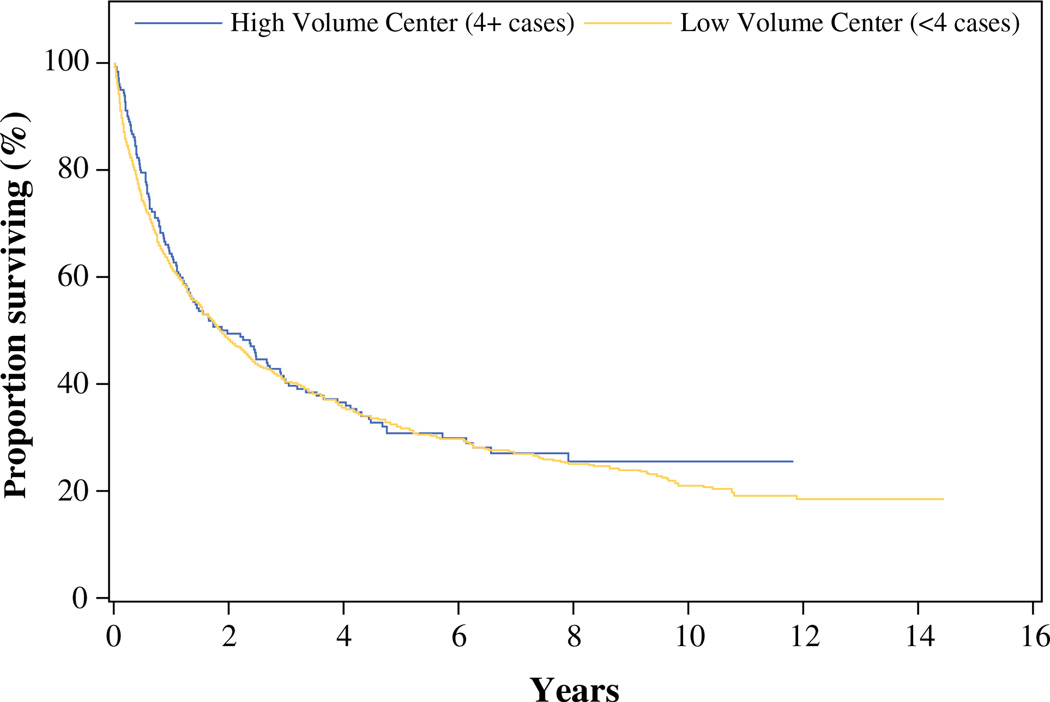
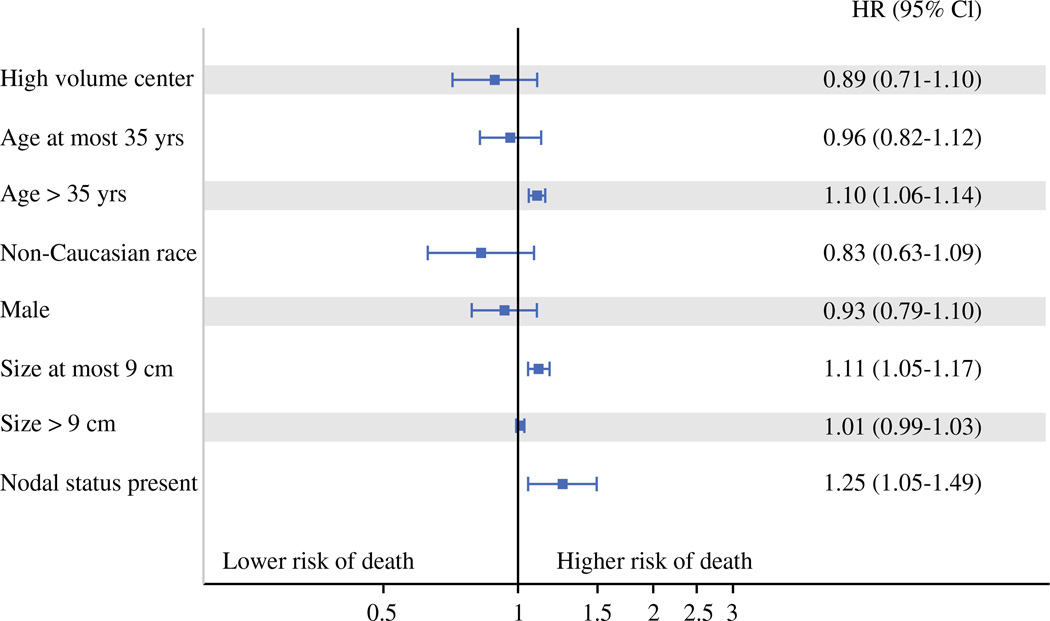
Results: A total of 2,765 ACC patients were treated across 1,046 facilities. Compared to patients treated at LVCs, patients treated at HVCs were younger (50 vs. 54 years), with larger tumors (11.2 vs. 10.5 cm), and underwent higher rates of surgery (78.8 vs. 73.4 %), radical resection (17.3 vs. 13.9 %), regional lymph node evaluation (23.2 vs. 18.8 %), and chemotherapy including mitotane (43.8 vs. 31.0 %, all p < 0.05).There were no significant differences in median length of stay (5 vs. 5 days), 30-day readmission rates (4.0 % for HVCs vs. 3.9 % for LVCs), or 30-day postoperative mortality rates (1.9 % for HVCs vs. 3.7 % for LVCs). Median overall survival was 2.0 years for HVCs and 1.9 years for LVCs, p = 0.53. After adjusting for patient and tumor characteristics, overall survival did not differ significantly between patients treated at HVCs versus LVCs [HR = 0.89 (95 % confidence interval 0.70, 1.12)].
Conclusions: Treatment at HVCs was associated with more aggressive surgical resection and chemotherapy use. Prognosis remained poor despite more aggressive treatment.
Figures
Comment in
-
Embracing national cancer registries for improved care of rare tumors.Ann Surg Oncol. 2014 Oct;21(11):3375-6. doi: 10.1245/s10434-014-3934-9. Epub 2014 Jul 26. Ann Surg Oncol. 2014. PMID: 25063007 Free PMC article. No abstract available.
-
Treatment Patterns and Outcomes for Patients with Adrenocortical Carcinoma Associated with Hospital Case Volume in the United States: A Reply.Ann Surg Oncol. 2017 Dec;24(Suppl 3):618. doi: 10.1245/s10434-017-6245-0. Epub 2017 Nov 13. Ann Surg Oncol. 2017. PMID: 29134376 No abstract available.
-
Treatment Patterns and Outcomes for Patients with Adrenocortical Carcinoma Associated with Hospital Case Volume in the United States.Ann Surg Oncol. 2017 Dec;24(Suppl 3):617. doi: 10.1245/s10434-017-6249-9. Epub 2017 Nov 16. Ann Surg Oncol. 2017. PMID: 29147927 No abstract available.
References
-
- Fassnacht M, Johanssen S, Quinkler M, et al. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a Revised TNM Classification. Cancer. 2009;115:243–250. - PubMed
-
- Pommier RF, Brennan MF. An eleven-year experience with adrenocortical carcinoma. Surgery. 1992;112:963–970. - PubMed
-
- Schulick RD, Brennan MF. Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann Surg Oncol. 1999;6:719–726. - PubMed
-
- Bellantone R, Ferrante A, Boscherini M, et al. Role of reoperation in recurrence of adrenal cortical carcinoma: results from 188 cases collected in the Italian National Registry for Adrenal Cortical Carcinoma. Surgery. 1997;122:1212–1218. - PubMed
-
- Icard P, Goudet P, Charpenay C, et al. Adrenocortical carcinomas: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons study group. World J Surg. 2001;25:891–897. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
