

Comprehensive biomarker testing of glycemia, insulin resistance, and beta cell function has greater sensitivity to detect diabetes risk than fasting glucose and HbA1c and is associated with improved glycemic control in clinical practice
- PMID: 25070680
- PMCID: PMC4137169
- DOI: 10.1007/s12265-014-9577-1
Comprehensive biomarker testing of glycemia, insulin resistance, and beta cell function has greater sensitivity to detect diabetes risk than fasting glucose and HbA1c and is associated with improved glycemic control in clinical practice
Abstract
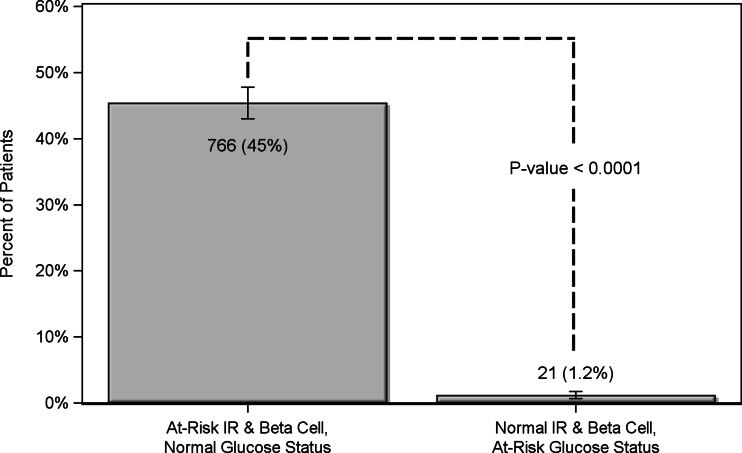
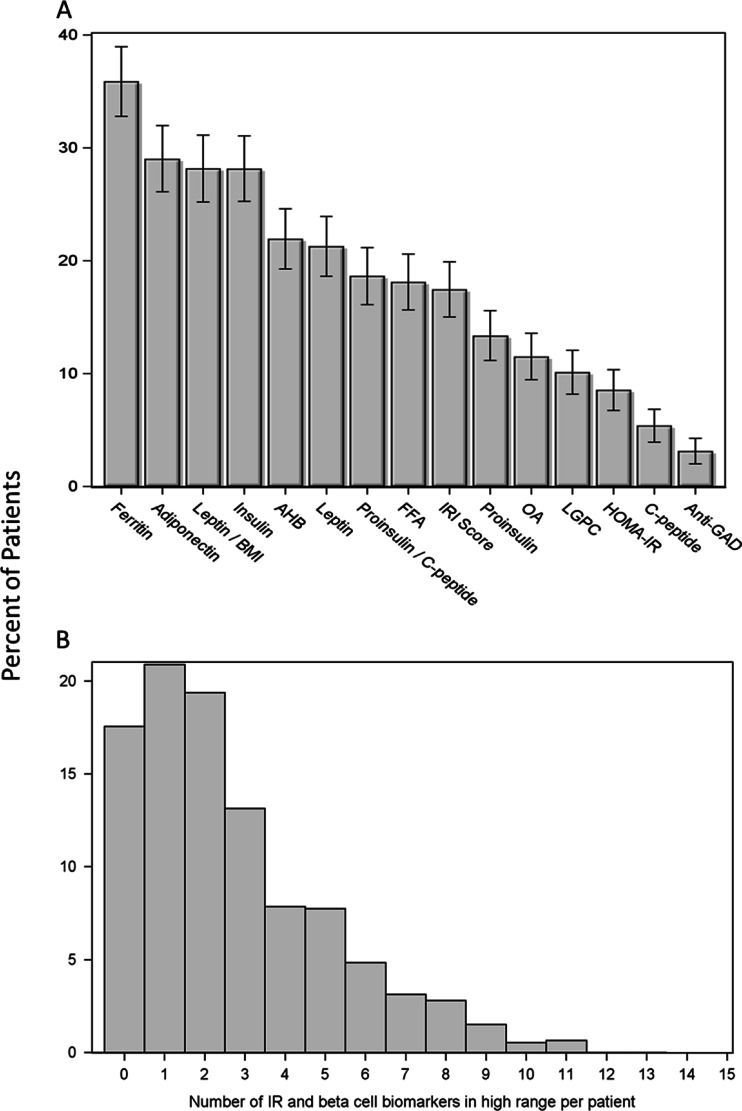
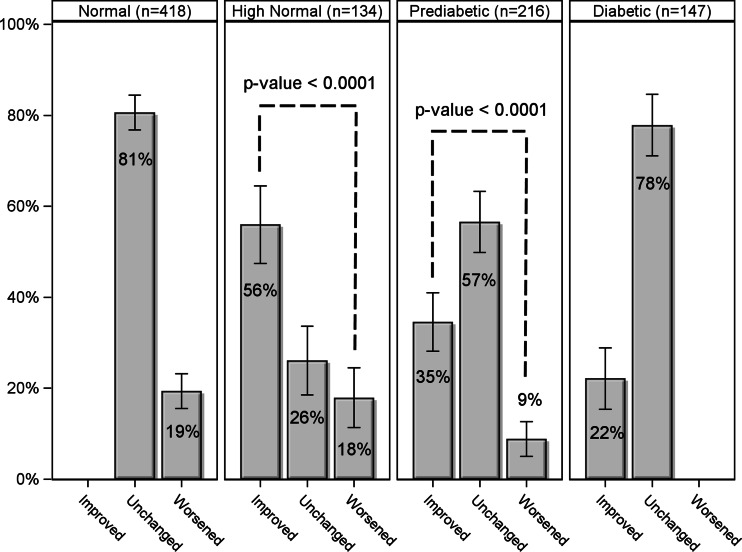
Blood-based biomarker testing of insulin resistance (IR) and beta cell dysfunction may identify diabetes risk earlier than current glycemia-based approaches. This retrospective cohort study assessed 1,687 US patients at risk for cardiovascular disease (CVD) under routine clinical care with a comprehensive panel of 19 biomarkers and derived factors related to IR, beta cell function, and glycemic control. The mean age was 53 ± 15, 42 % were male, and 25 % had glycemic indicators consistent with prediabetes. An additional 45 % of the patients who had normal glycemic indicators were identified with IR or beta cell abnormalities. After 5.3 months of median follow-up, significantly more patients had improved than worsened their glycemic status in the prediabetic category (35 vs. 9 %; P < 0.0001) and in the "high normal" category (HbA1c values of 5.5-5.6; 56 vs. 18 %, p < 0.0001). Biomarker testing can identify IR early, enable and inform treatment, and improve glycemic control in a high proportion of patients.
Conflict of interest statement
All authors employed by Health Diagnostic Laboratory, Inc., share a potential conflict of interest since this laboratory offers the referenced biomarker testing commercially. Timothy Graham has received consulting fees from Health Diagnostic Laboratory, Inc.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). (2011). National diabetes fact sheet. Atlanta, Georgia.
-
- International Diabetes Federation (2013). IDF Diabetes Atlas, 6th edn. Brussels, Belgium: International Diabetes Federation. http://www.idf.org/diabetesatlas/global-burden. Accessed 24 July 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
