

Monocytes and macrophages in pregnancy and pre-eclampsia
- PMID: 25071761
- PMCID: PMC4074993
- DOI: 10.3389/fimmu.2014.00298
Monocytes and macrophages in pregnancy and pre-eclampsia
Abstract
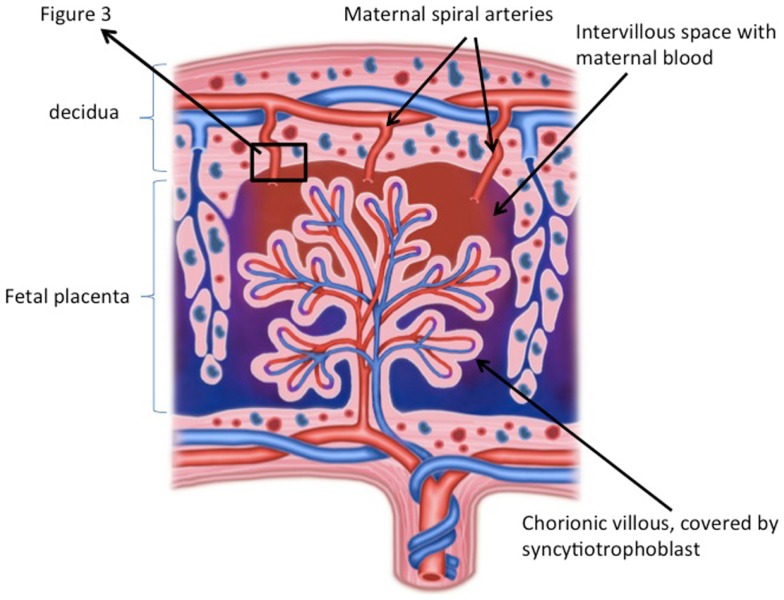
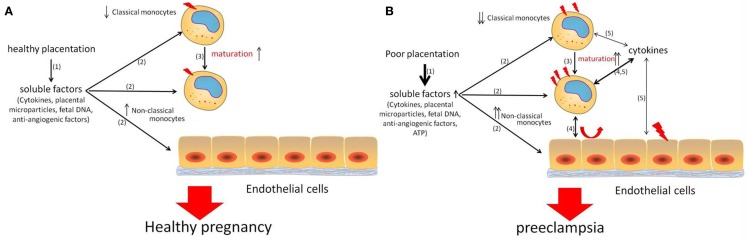
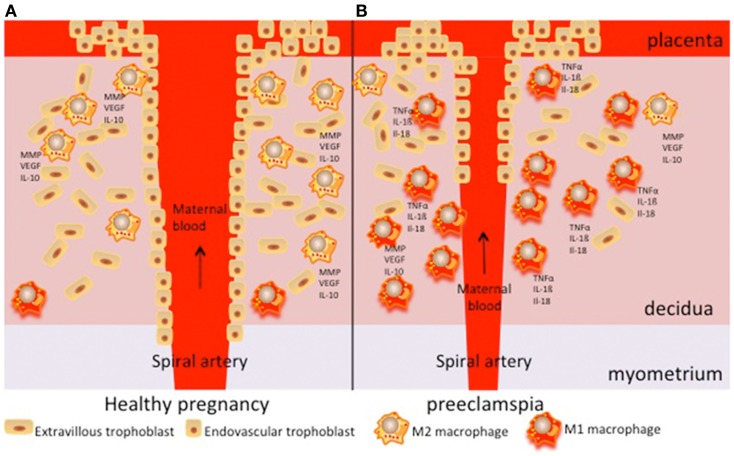
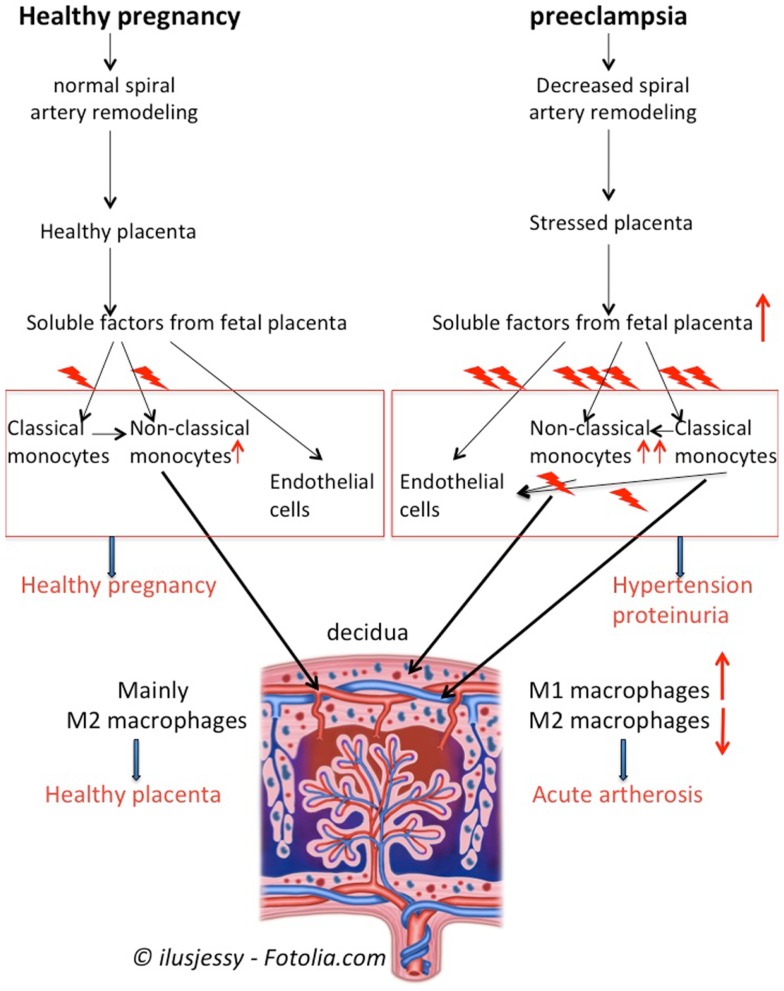
Preeclampsia is an important complication in pregnancy, characterized by hypertension and proteinuria in the second half of pregnancy. Generalized activation of the inflammatory response is thought to play a role in the pathogenesis of pre-eclampsia. Monocytes may play a central role in this inflammatory response. Monocytes are short lived cells that mature in the circulation and invade into tissues upon an inflammatory stimulus and develop into macrophages. Macrophages are abundantly present in the endometrium and play a role in implantation and placentation in normal pregnancy. In pre-eclampsia, these macrophages appear to be present in larger numbers and are also activated. In the present review, we focused on the role of monocytes and macrophages in the pathophysiology of pre-eclampsia.
Keywords: decidua; macrophages; monocytes; placenta; pre-eclampsia; pregnancy.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources