

Urinary Continence Following Repair of Intermediate and High Urogenital Sinus (UGS) in CAH. Experience with 55 Cases
- PMID: 25072036
- PMCID: PMC4078913
- DOI: 10.3389/fped.2014.00067
Urinary Continence Following Repair of Intermediate and High Urogenital Sinus (UGS) in CAH. Experience with 55 Cases
Abstract
Aim: To evaluate postoperative urinary continence in patients with congenital adrenal hyperplasia (CAH) with intermediate (IT) and high urogenital sinus (UGS) who underwent a UGS mobilization maneuver.
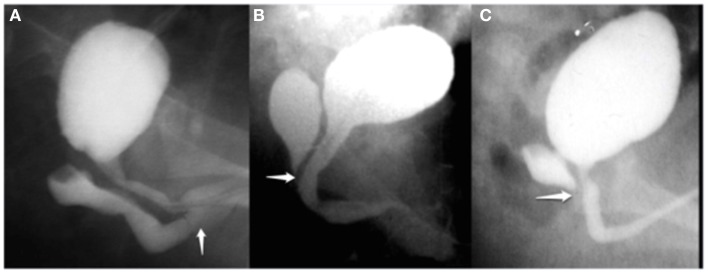
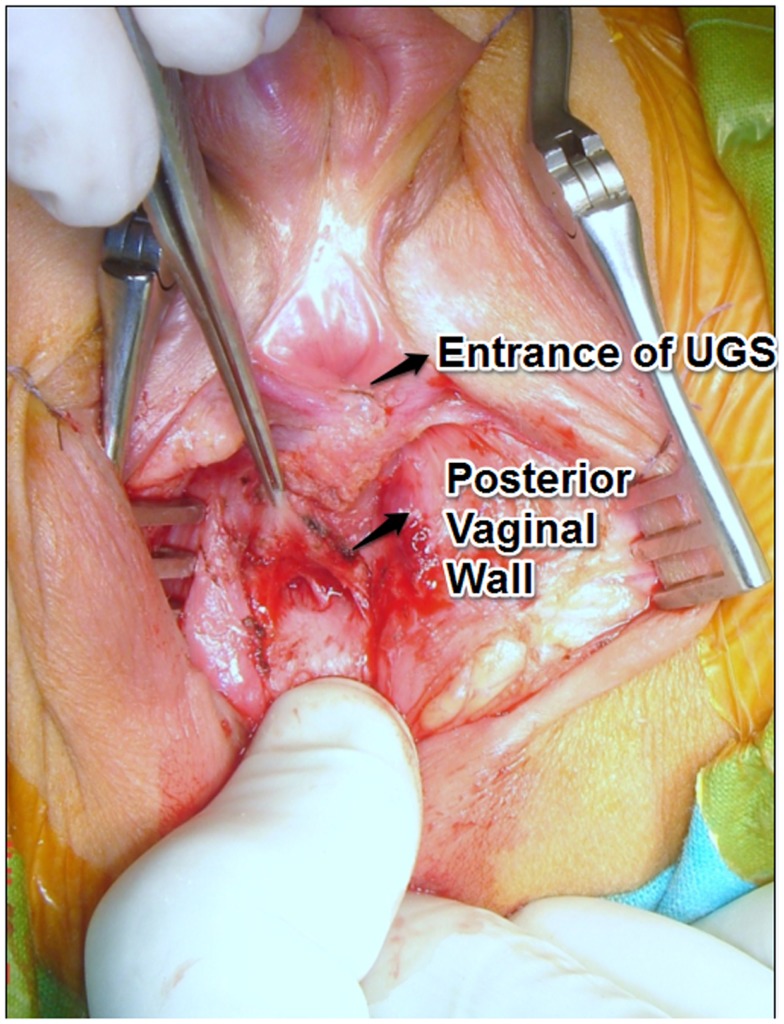
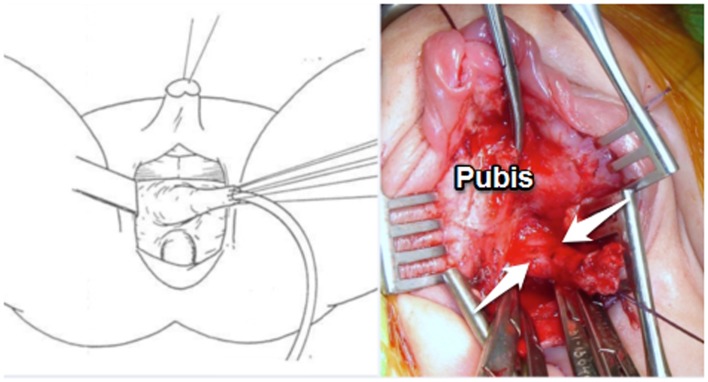
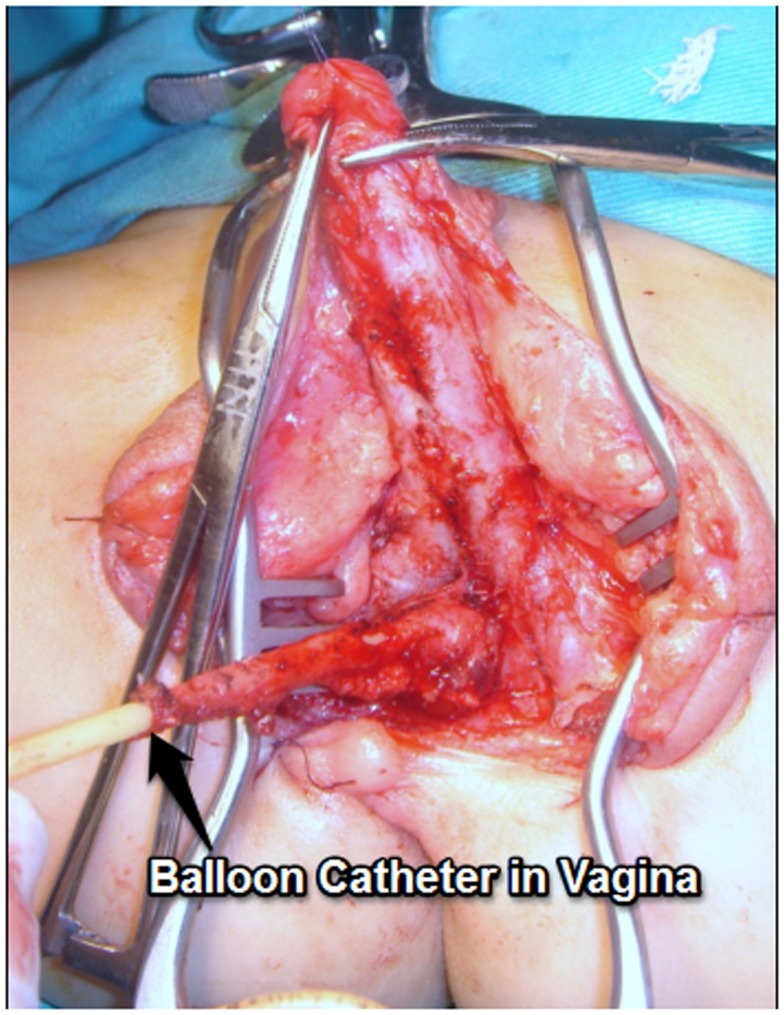
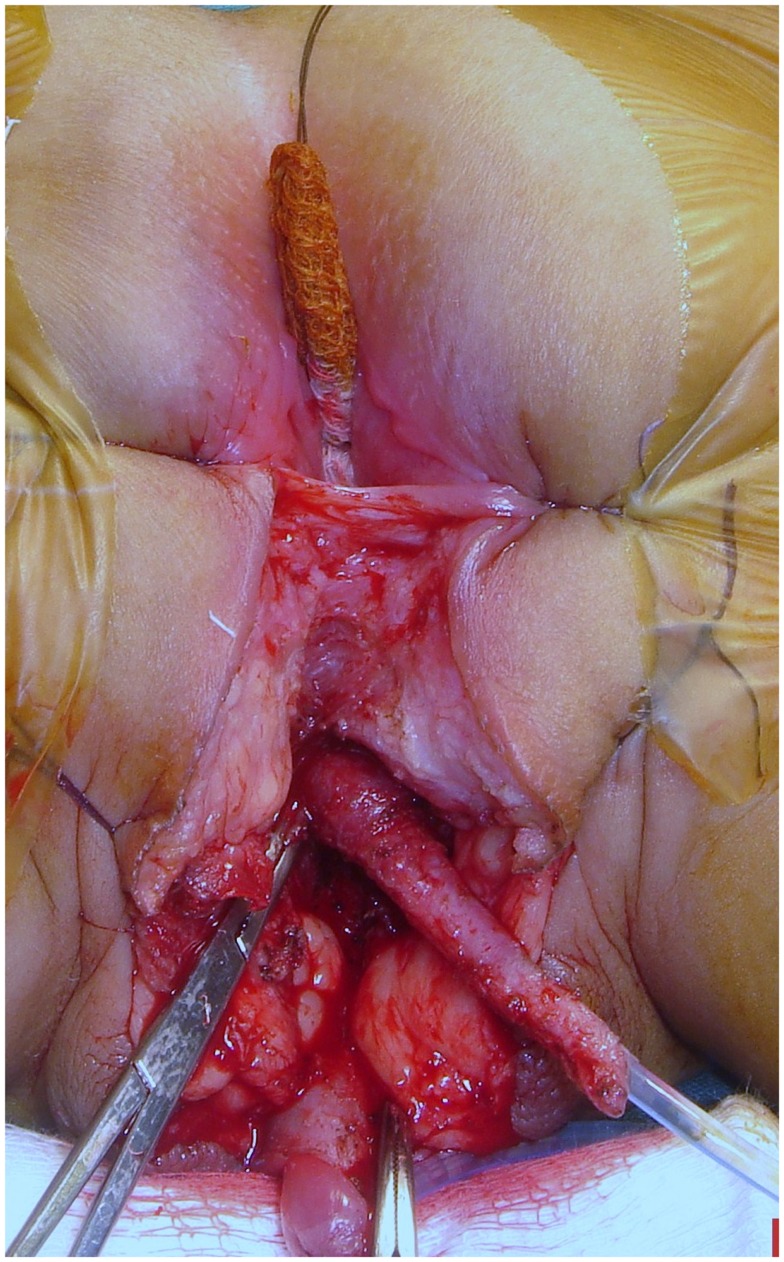
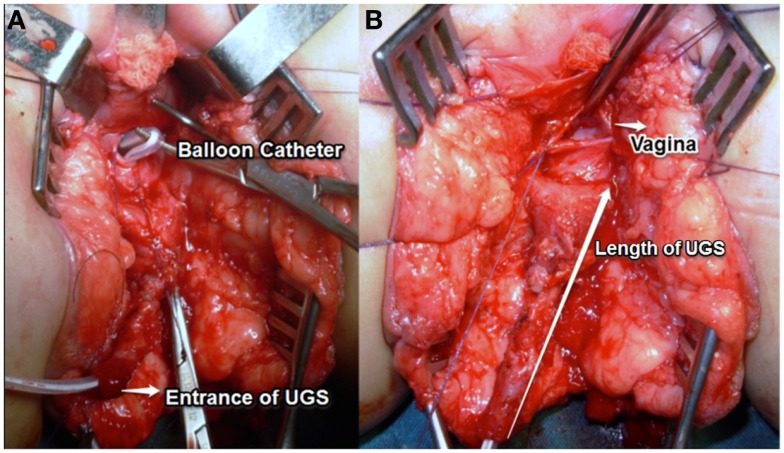
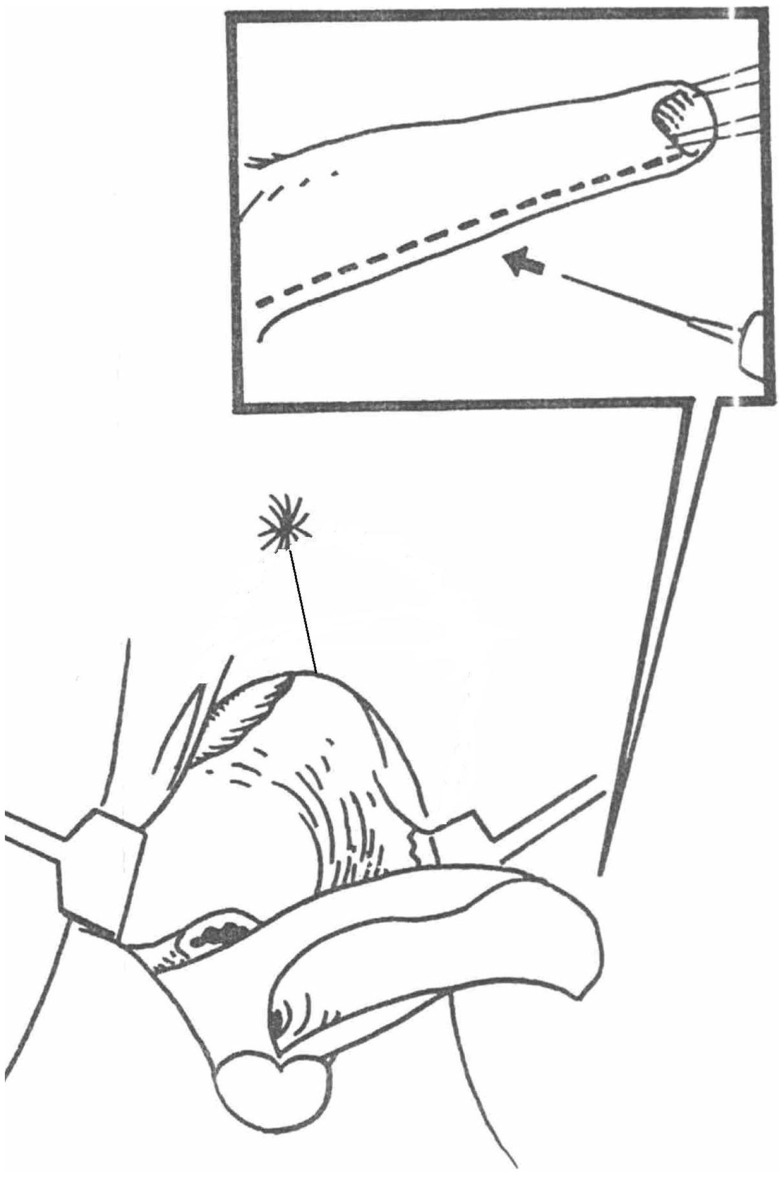
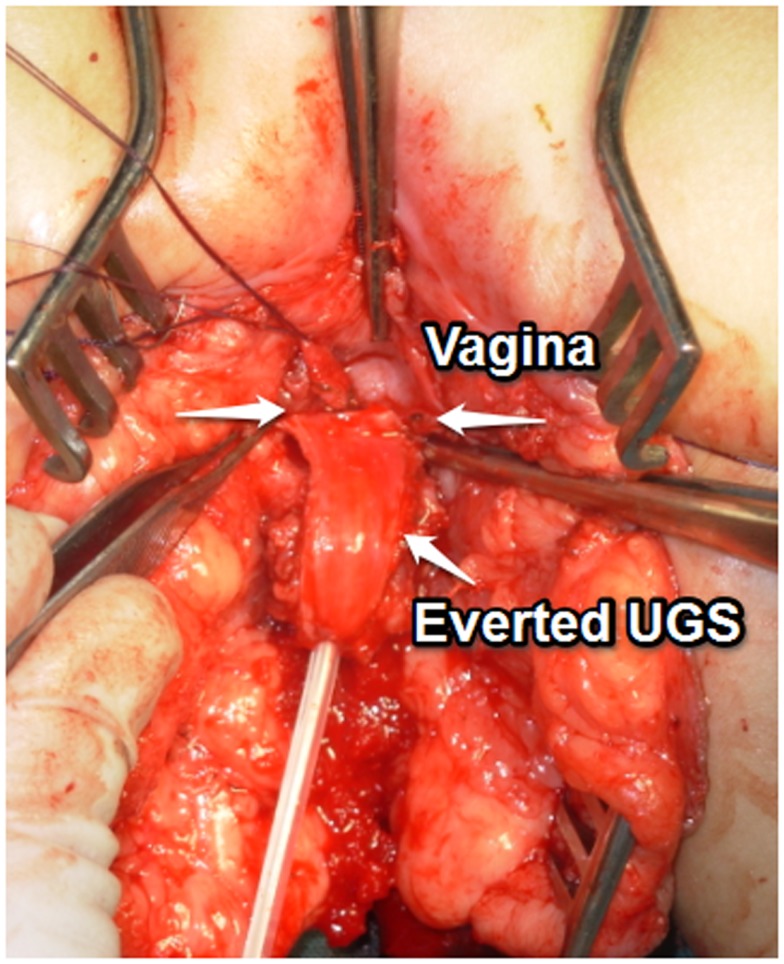
Methods: We called IT to those that although needing an aggressive dissection to get to the vagina, still have enough urethra proximal to the vaginal confluence. Very low variants are excluded from this analysis. Dissection always started in the posterior wall of the UGS with an aggressive separation from the anterior rectal wall. If the wide portion of the vagina was reached dissection stopped and the UGS opened ventrally widening to the introitus. Nineteen patients were treated using this maneuver (Group 1). When more dissection was required the anterior wall of the UGS was dissected and carefully freed from the low retropubic space. Then the UGS was opened either ventrally or dorsally. Thirty three patients required this approach (Group 2). Combined procedures were used in three patients with high UGS (Group 3).
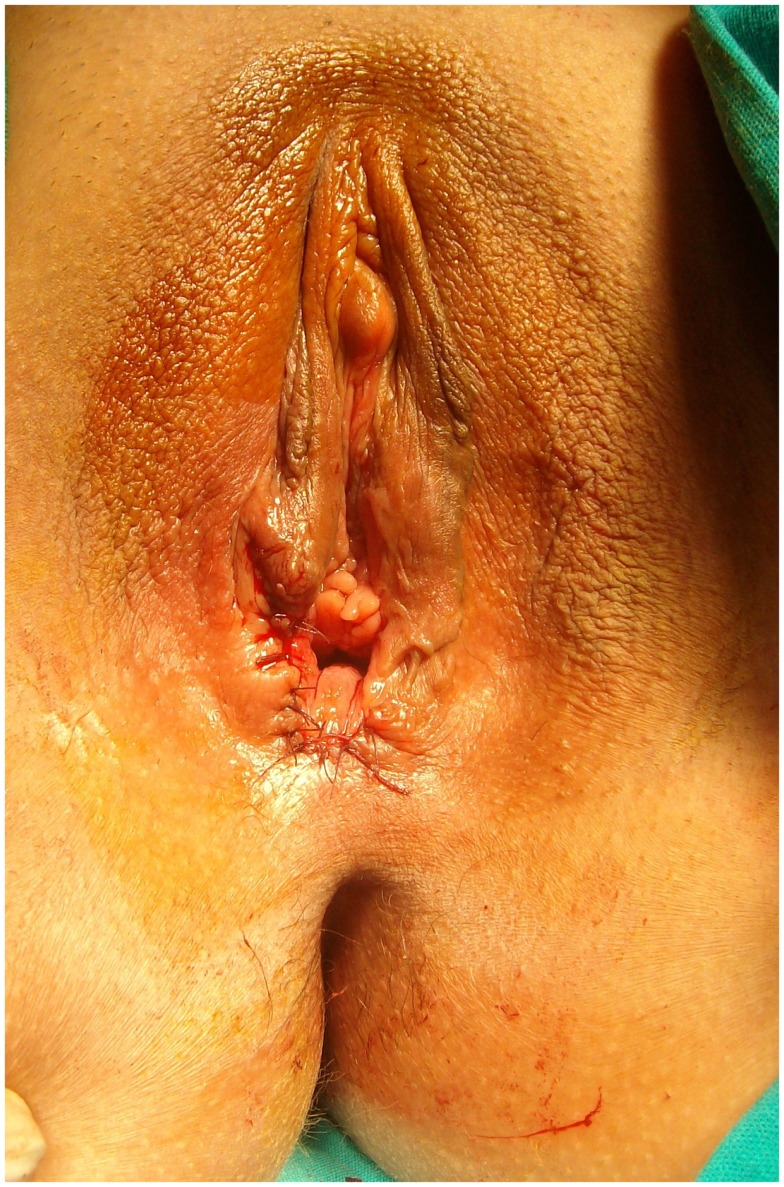
Results: Mean age at the time of the repair and length of the UGS were 12.2 years (4 months-18 years) and 3.75 cm (3-8 cm) for G1; 8 years (5 months-17 years) and 6.34 cm (4-12 cm) in G2 and 8.3 years (2-14 years) and 11.5 cm (11-12 cm) in G3. All patients had been regularly followed. Mean age at last follow up was 14.3, 17, and 9.9 years for Groups 1, 2, and 3, respectively. All patients continue to void normally and are continent. All patients have two separate visible orifices in the vulva. Only three are sexually active.
Conclusion: Urogenital sinus mobilization for vaginoplasty in girls with CAH does not compromise voiding function or urinary continence.
Keywords: congenital adrenal hyperplasia; high urogenital sinus; intermediate urogenital sinus; urinary continence after urogenital reconstruction; urogenital sinus mobilization.
Figures
References
-
- Bailez M, Fraire C. Total mobilization of the urogenital sinus for the treatment of adrenal hyperplasia. ESPU; Salzburg, Austria: (1998) 81:76 [Abstract in BJU].
LinkOut - more resources
Full Text Sources
Other Literature Sources