

Inflammatory response in mixed viral-bacterial community-acquired pneumonia
- PMID: 25073709
- PMCID: PMC4118651
- DOI: 10.1186/1471-2466-14-123
Inflammatory response in mixed viral-bacterial community-acquired pneumonia
Abstract
Background: The role of mixed pneumonia (virus+bacteria) in community-acquired pneumonia (CAP) has been described in recent years. However, it is not known whether the systemic inflammatory profile is different compared to monomicrobial CAP. We wanted to investigate this profile of mixed viral-bacterial infection and to compare it to monomicrobial bacterial or viral CAP.
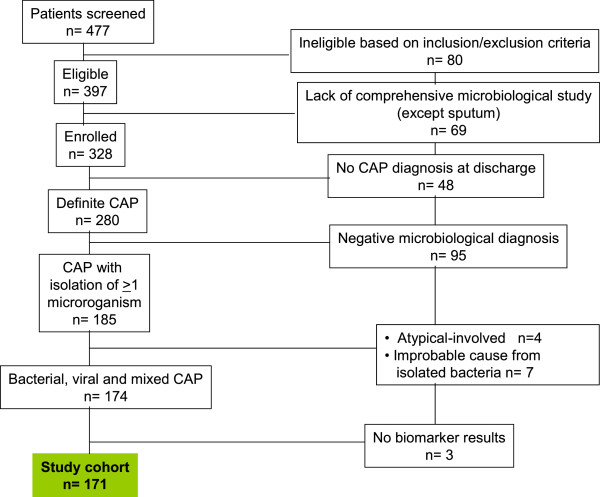
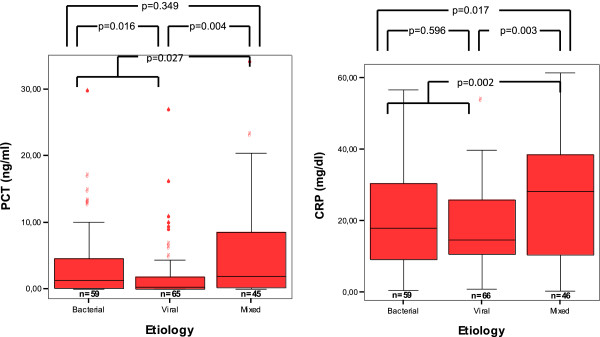
Methods: We measured baseline serum procalcitonin (PCT), C reactive protein (CRP), and white blood cell (WBC) count in 171 patients with CAP with definite etiology admitted to a tertiary hospital: 59 (34.5%) bacterial, 66 (39.%) viral and 46 (27%) mixed (viral-bacterial).
Results: Serum PCT levels were higher in mixed and bacterial CAP compared to viral CAP. CRP levels were higher in mixed CAP compared to the other groups. CRP was independently associated with mixed CAP. CRP levels below 26 mg/dL were indicative of an etiology other than mixed in 83% of cases, but the positive predictive value was 45%. PCT levels over 2.10 ng/mL had a positive predictive value for bacterial-involved CAP versus viral CAP of 78%, but the negative predictive value was 48%.
Conclusions: Mixed CAP has a different inflammatory pattern compared to bacterial or viral CAP. High CRP levels may be useful for clinicians to suspect mixed CAP.
Figures


References
-
- Jennings LC, Anderson TP, Beynon KA, Chua A, Laing RTR, Werno AM, Young SA, Chambers ST, Murdoch DR. Incidence and characteristics of viral community-acquired pneumonia in adults. Thorax. 2008;63:42–48. - PubMed
-
- Marcos MA, Camps M, Pumarola T, Martinez JA, Martinez E, Mensa J, Garcia E, Peñarroja G, Dambrava P, Casas I, de Jiménez Anta MT, Torres A. The role of viruses in the aetiology of community-acquired pneumonia in adults. Antivir Ther. 2006;11:351–359. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
