

Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems
- PMID: 25074069
- PMCID: PMC4134114
- DOI: 10.1186/1471-2415-14-96
Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems
Abstract
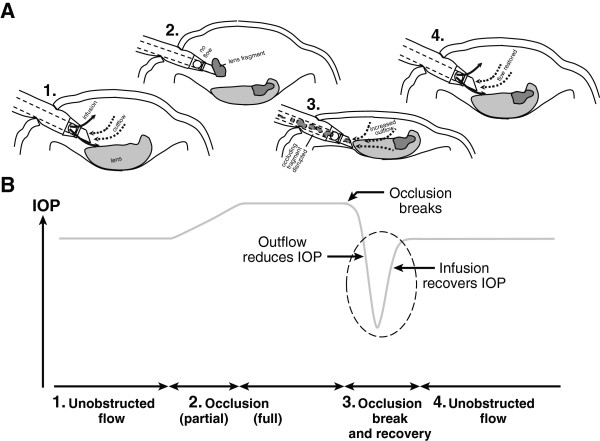
Background: Occlusion break surge during phacoemulsification cataract surgery can lead to potential surgical complications. The purpose of this study was to quantify occlusion break surge and vacuum rise time of current phacoemulsification systems used in cataract surgery.
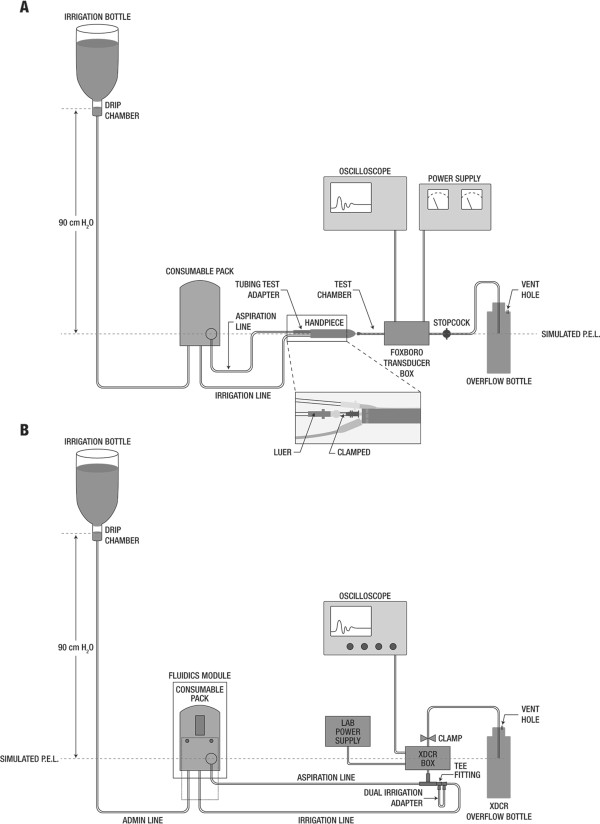
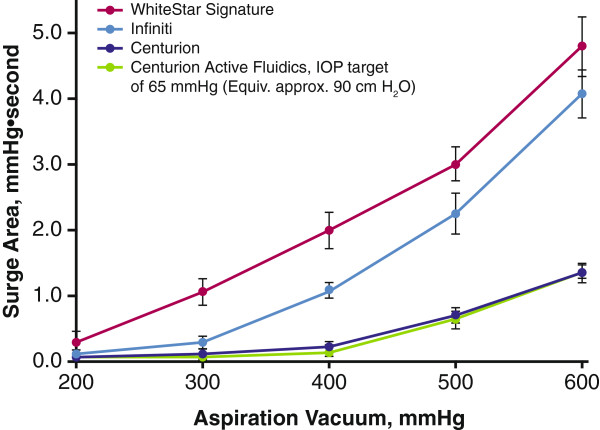
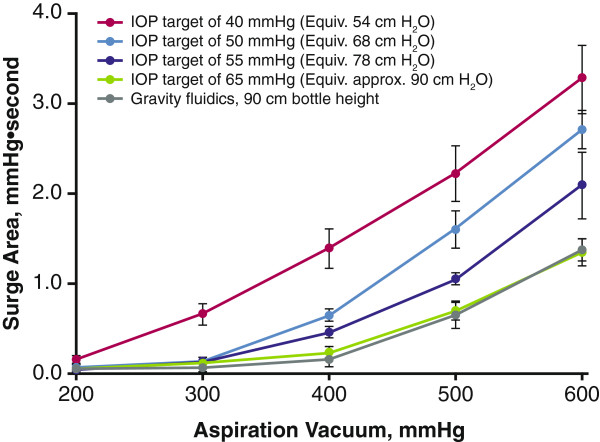
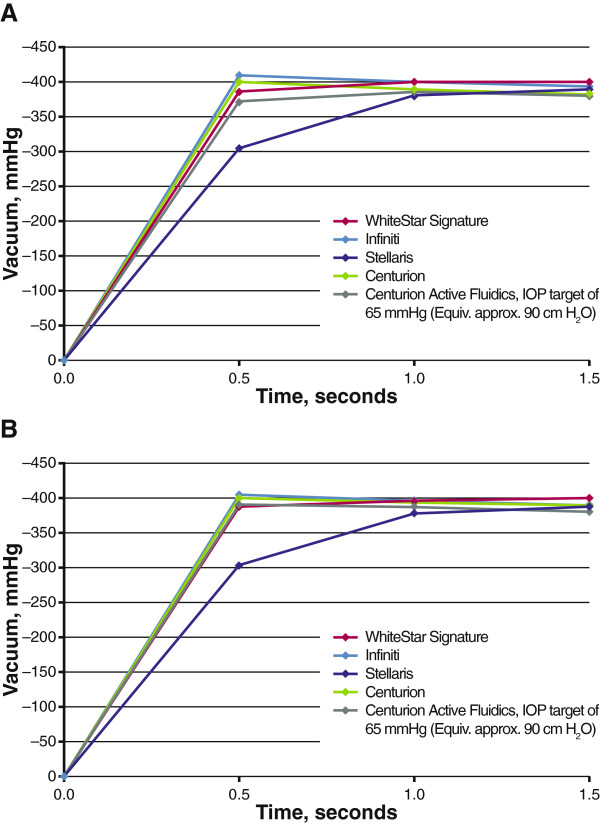
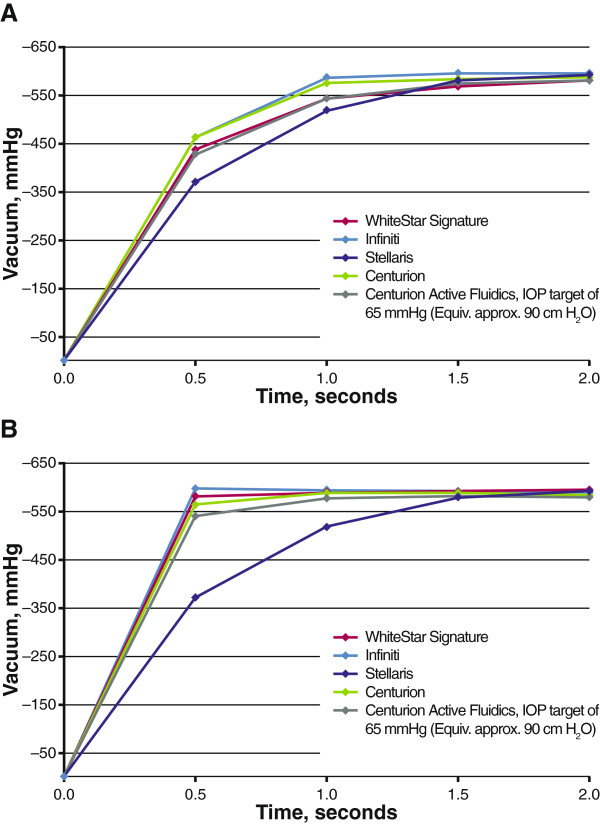
Methods: Occlusion break surge at vacuum pressures between 200 and 600 mmHg was assessed with the Infiniti® Vision System, the WhiteStar Signature® Phacoemulsification System, and the Centurion® Vision System using gravity-fed fluidics. Centurion Active FluidicsTM were also tested at multiple intraoperative pressure target settings. Vacuum rise time was evaluated for Infiniti, WhiteStar Signature, Centurion, and Stellaris® Vision Enhancement systems. Rise time to vacuum limits of 400 and 600 mmHg was assessed at flow rates of 30 and 60 cc/minute. Occlusion break surge was analyzed by 2-way analysis of variance.
Results: The Centurion system exhibited substantially less occlusion break surge than the other systems tested. Surge area with Centurion Active Fluidics was similar to gravity fluidics at an equivalent bottle height. At all Centurion Active Fluidics intraoperative pressure target settings tested, surge was smaller than with Infiniti and WhiteStar Signature. Infiniti had the fastest vacuum rise time and Stellaris had the slowest. No system tested reached the 600-mmHg vacuum limit.
Conclusions: In this laboratory study, Centurion had the least occlusion break surge and similar vacuum rise times compared with the other systems tested. Reducing occlusion break surge may increase safety of phacoemulsification cataract surgery.
Figures
References
-
- Congdon N, Vingerling JR, Klein BE, West S, Friedman DS, Kempen J, O’Colmain B, Wu SY, Taylor HR. Eye Diseases Prevalence Research Group. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol. 2004;122(4):487–494. - PubMed
-
- Khanna R, Pujari S, Sangwan V. Cataract surgery in developing countries. Curr Opin Ophthalmol. 2011;22(1):10–14. - PubMed
-
- Blindness: Vision 2020 - Control of Major Blinding Diseases and Disorders. The Global Initiative for the Elimination of Avoidable Blindness, fact sheet No. 214. [ http://www.who.int/mediacentre/factsheets/fs214/en/]
-
- Lundstrom M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European Registry of Quality Outcomes for Cataract and Refractive Surgery database. J Cataract Refract Surg. 2012;38(6):1086–1093. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
