

A randomized study of contingency management and spirometric lung age for motivating smoking cessation among injection drug users
- PMID: 25074396
- PMCID: PMC4132916
- DOI: 10.1186/1471-2458-14-761
A randomized study of contingency management and spirometric lung age for motivating smoking cessation among injection drug users
Abstract
Background: Even after quitting illicit drugs, tobacco abuse remains a major cause of morbidity and mortality in former injection drug users. An important unmet need in this population is to have effective interventions that can be used in the context of community based care. Contingency management, where a patient receives a monetary incentive for healthy behavior choices, and incorporation of individual counseling regarding spirometric "lung age" (the age of an average healthy individual with similar spirometry) have been shown to improve cessation rates in some populations. The efficacy of these interventions on improving smoking cessation rates has not been studied among current and former injection drug users.
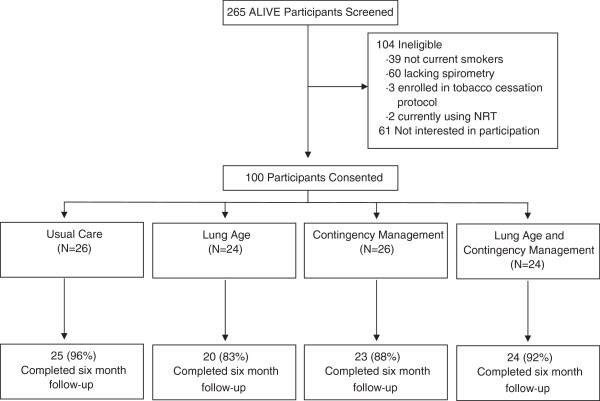
Methods: In a randomized, factorial design study, we recruited 100 active smokers from an ongoing cohort study of current and former injection drug users to assess the impact of contingency management and spirometric lung age on smoking cessation. The primary outcome was 6-month biologically-confirmed smoking cessation comparing contingency management, spirometric lung age or both to usual care. Secondary outcomes included differences in self-reported and biologically-confirmed cessation at interim visits, number of visits attended and quit attempts, smoking rates at interim visits, and changes in Fagerstrom score and self-efficacy.
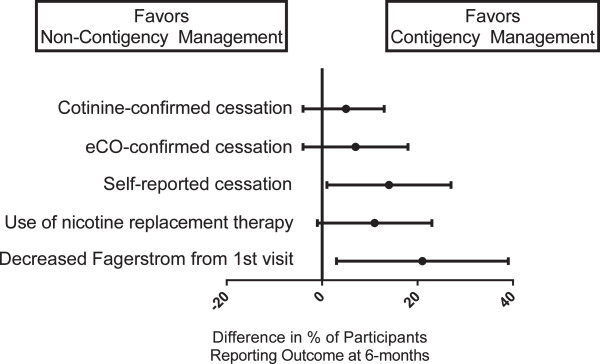
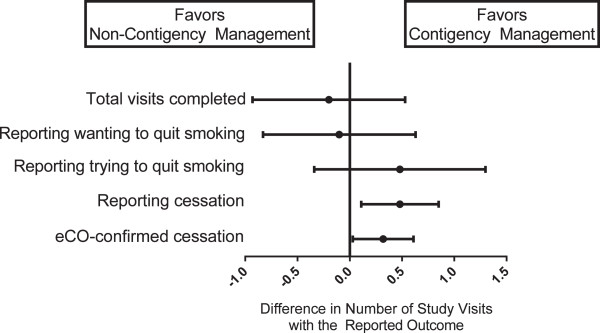
Results: Six-month biologically-confirmed smoking cessations rates were 4% usual care, 0% lung age, 14% contingency management and 0% for combined lung age and contingency management (p = 0.13). There were no differences in secondary endpoints comparing the four interventions or when pooling the lung age groups. Comparing contingency management to non-contingency management, 6-month cessation rates were not different (7% vs. 2%; p = 0.36), but total number of visits with exhaled carbon monoxide-confirmed abstinence were higher for contingency management than non-contingency management participants (0.38 vs. 0.06; p = 0.03), and more contingency management participants showed reduction in their Fagerstrom score from baseline to follow-up (39% vs. 18%; p = 0.03).
Conclusions: While lung age appeared ineffective, contingency management was associated with more short-term abstinence and lowered nicotine addiction. Contingency management may be a useful tool in development of effective tobacco cessation strategies among current and former injection drug users.
Trial registration: Clinicaltrials.gov NCT01334736 (April 12, 2011).
Figures
References
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/761/prepub
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
