

Non-ST-elevation myocardial infarction in the United States: contemporary trends in incidence, utilization of the early invasive strategy, and in-hospital outcomes
- PMID: 25074695
- PMCID: PMC4310389
- DOI: 10.1161/JAHA.114.000995
Non-ST-elevation myocardial infarction in the United States: contemporary trends in incidence, utilization of the early invasive strategy, and in-hospital outcomes
Abstract
Background: There has been a paradigm shift in the definition of timing of early invasive strategy (EIS) for patients admitted with non-ST-elevation myocardial infarction (NSTEMI) in the last decade. Data on trends of EIS for NSTEMI and associated in-hospital outcomes are limited. Our aim is to analyze temporal trends in the incidence, utilization of early invasive strategy, and in-hospital outcomes of NSTEMI in the United States.
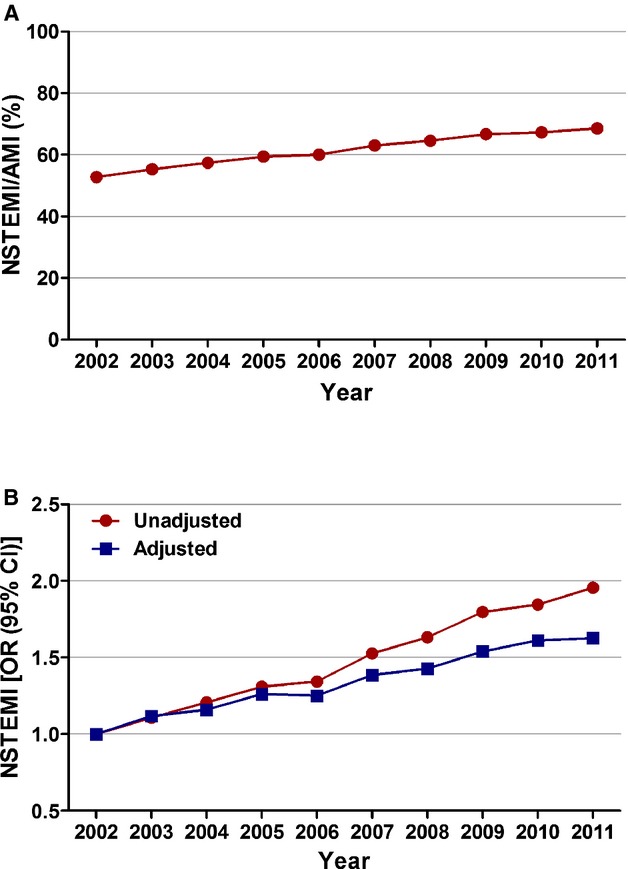
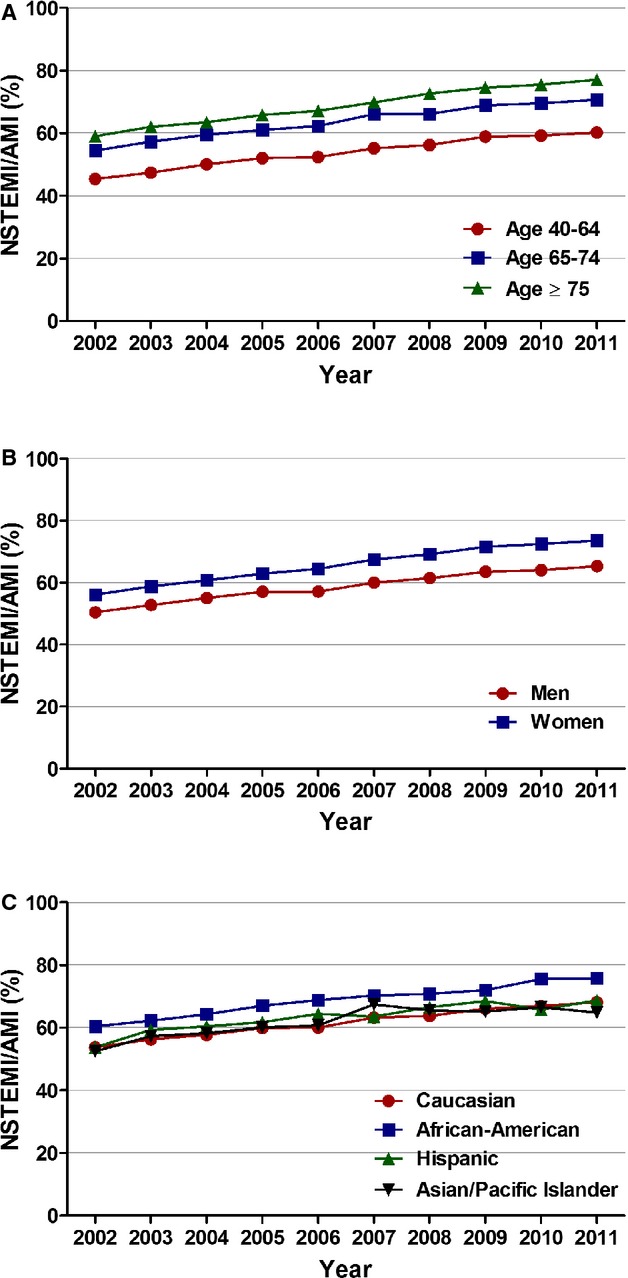
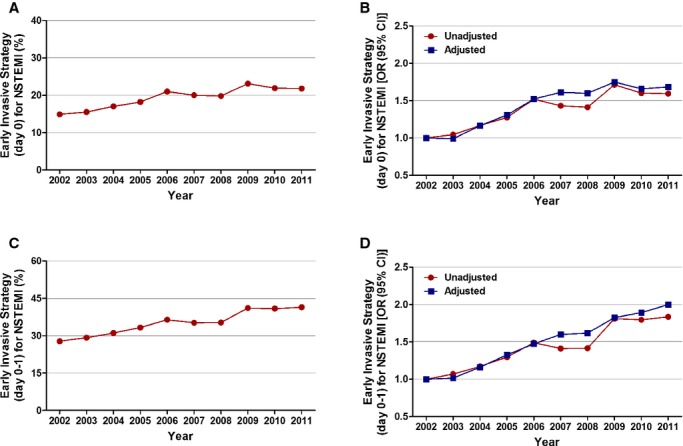
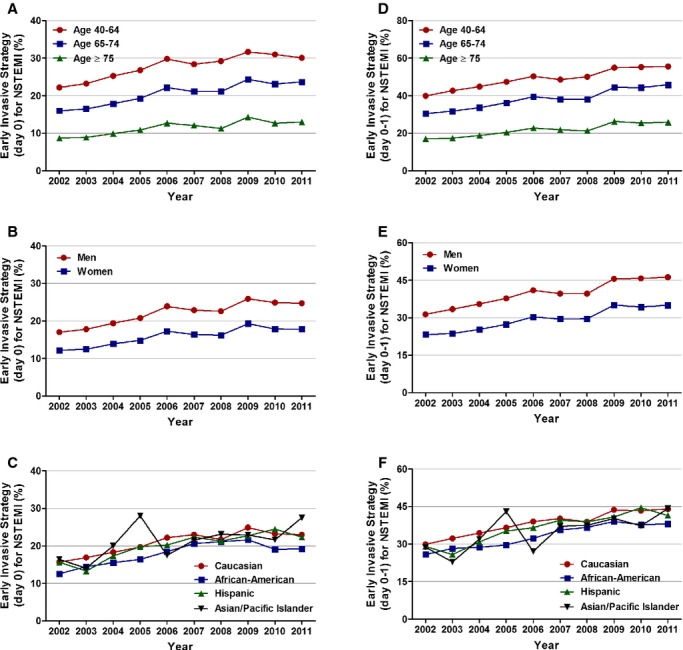
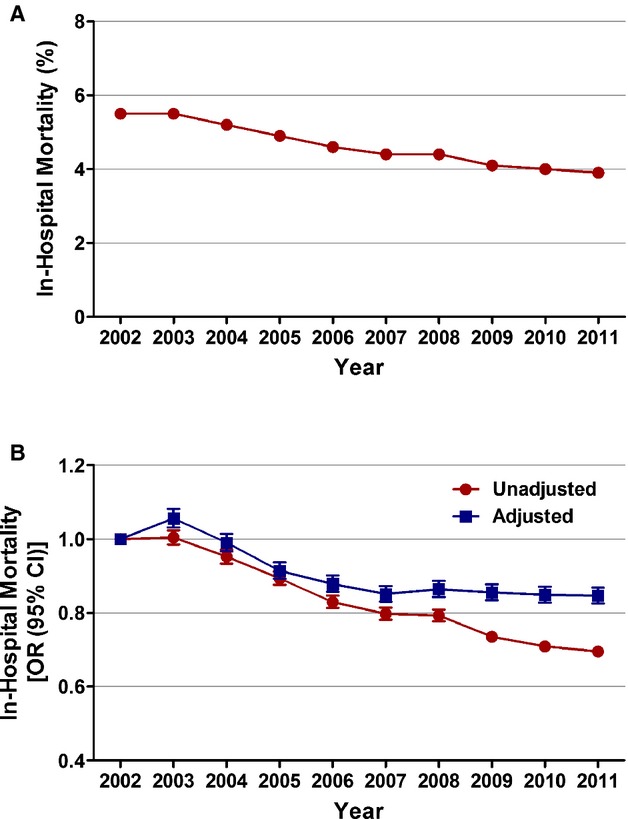
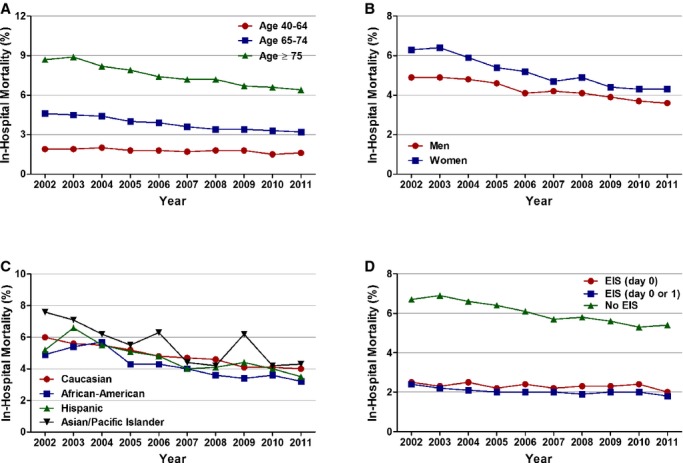
Methods and results: We analyzed the 2002-2011 Nationwide Inpatient Sample databases to identify all patients ≥40 years of age with the principal diagnosis of acute myocardial infarction (AMI) and NSTEMI. Logistic regression was used for overall, age-, sex-, and race/ethnicity-stratified trend analysis. From 2002 to 2011, we identified 6 512 372 patients with AMI. Of these, 3 981 119 (61.1%) had NSTEMI. The proportion of patients with NSTEMI increased from 52.8% in 2002 to 68.6% in 2011 (adjusted odds ratio [OR; per year], 1.055; 95% confidence interval [CI], 1.054 to 1.056) in the overall cohort. Similar trends were observed in age-, sex-, and race/ethnicity-stratified groups. From 2002 to 2011, utilization of EIS at day 0 increased from 14.9% to 21.8% (Ptrend<0.001) and utilization of EIS at day 0 or 1 increased from 27.8% to 41.4% (Ptrend<0.001). Risk-adjusted in-hospital mortality in the overall cohort decreased during the study period (adjusted OR [per year], 0.976; 95% CI, 0.974 to 0.978).
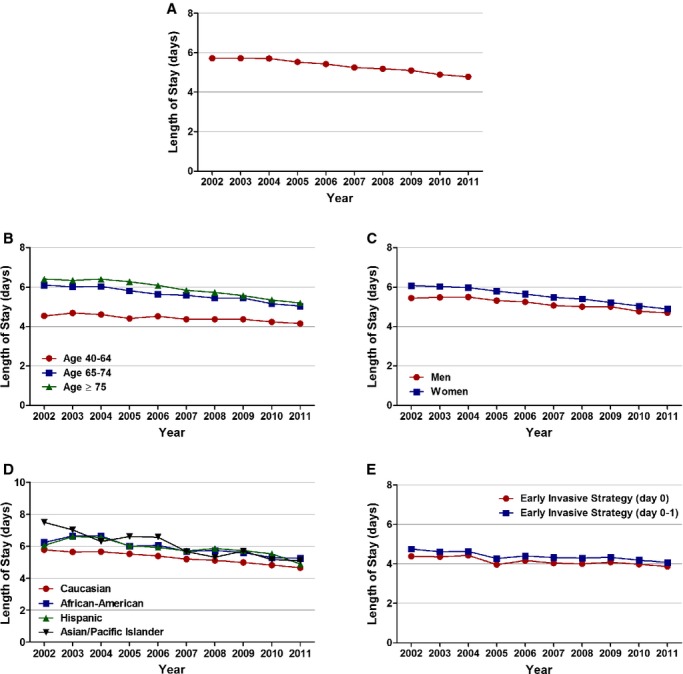
Conclusions: There have been temporal increases in the proportion of NSTEMI and, consistent with guidelines, greater utilization of EIS. This has been accompanied by temporal decreases in in-hospital mortality and length of stay.
Keywords: early invasive strategy; in‐hospital mortality; non‐ST‐elevation myocardial infarction; temporal trends.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Roger VL, Go AS, Lloyd‐Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MBon behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2012 update: a report from the American Heart Association. Circulation. 2012; 125:e2-e220. - PMC - PubMed
-
- Rogers WJ, Frederick PD, Stoehr E, Canto JG, Ornato JP, Gibson CM, Pollack CV, Gore JM, Chandra‐Strobos N, Peterson ED, French WJ. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non‐ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008; 156:1026-1034. - PubMed
-
- Khera S, Kolte D, Palaniswamy C, Mujib M, Aronow WS, Singh T, Gotsis W, Silverman G, Frishman WH. ST‐elevation myocardial infarction in the elderly—temporal trends in incidence, utilization of percutaneous coronary intervention and outcomes in the United States. Int J Cardiol. 2013; 168:3683-3690. - PubMed
-
- Jennings SM, Bennett K, Lonergan M, Shelley E. Trends in hospitalisation for acute myocardial infarction in Ireland, 1997–2008. Heart. 2012; 98:1285-1289. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
