

Remote ischemic preconditioning in children undergoing cardiac surgery with cardiopulmonary bypass: a single-center double-blinded randomized trial
- PMID: 25074698
- PMCID: PMC4310383
- DOI: 10.1161/JAHA.114.000964
Remote ischemic preconditioning in children undergoing cardiac surgery with cardiopulmonary bypass: a single-center double-blinded randomized trial
Abstract
Background: Remote ischemic preconditioning (RIPC) harnesses an innate defensive mechanism that protects against inflammatory activation and ischemia-reperfusion injury, known sequelae of cardiac surgery with cardiopulmonary bypass. We sought to determine the impact of RIPC on clinical outcomes and physiological markers related to ischemia-reperfusion injury and inflammatory activation after cardiac surgery in children.
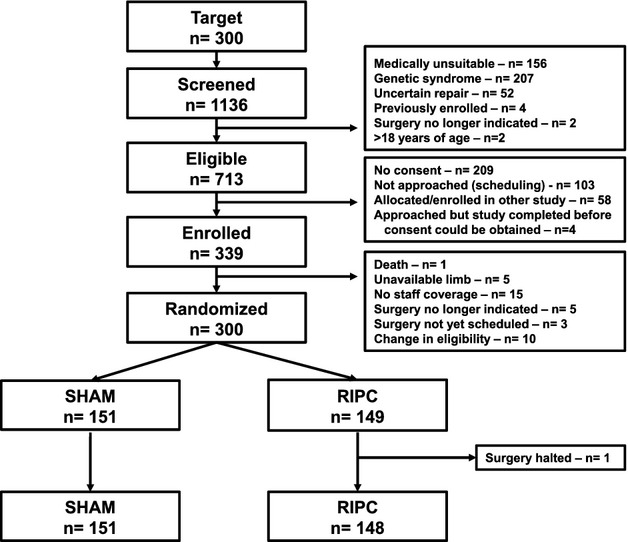
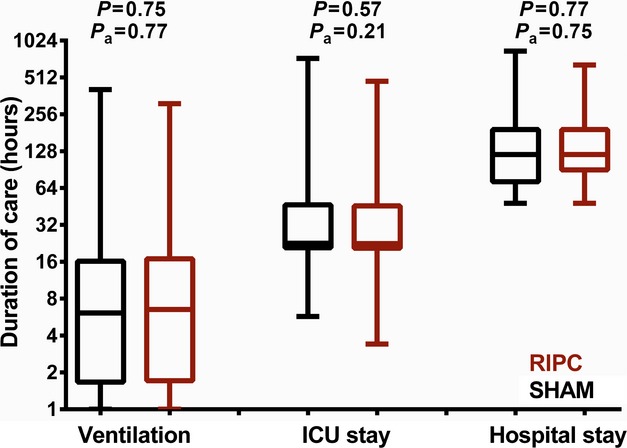
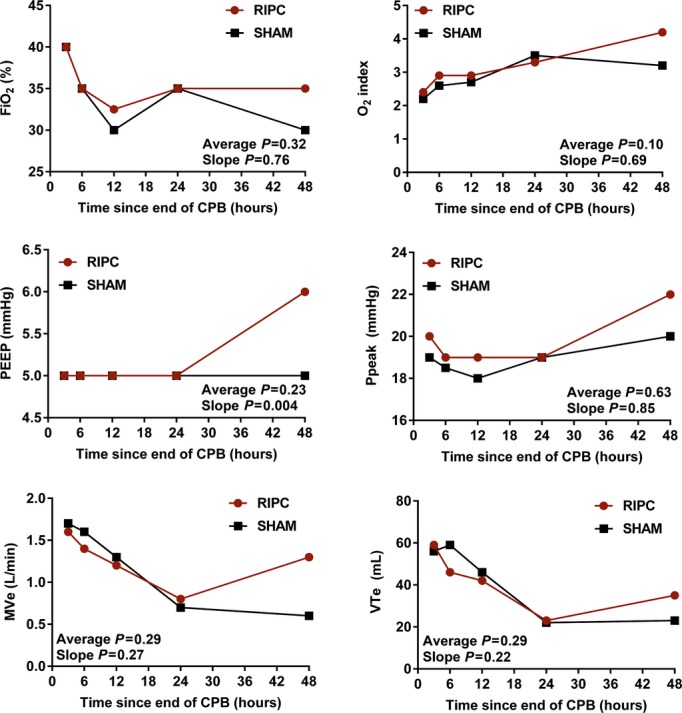
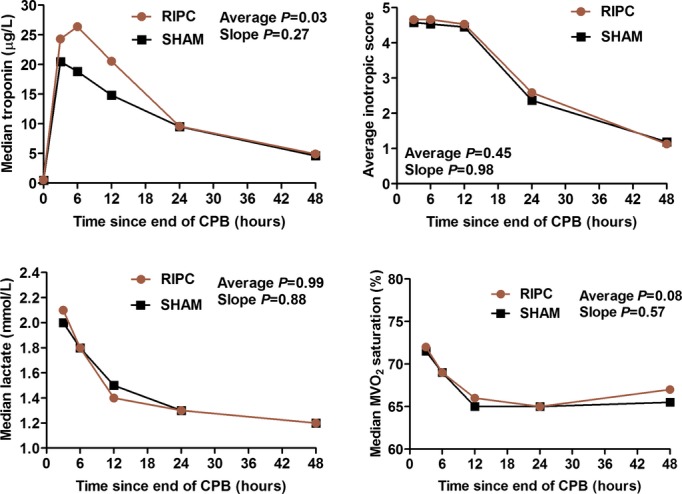
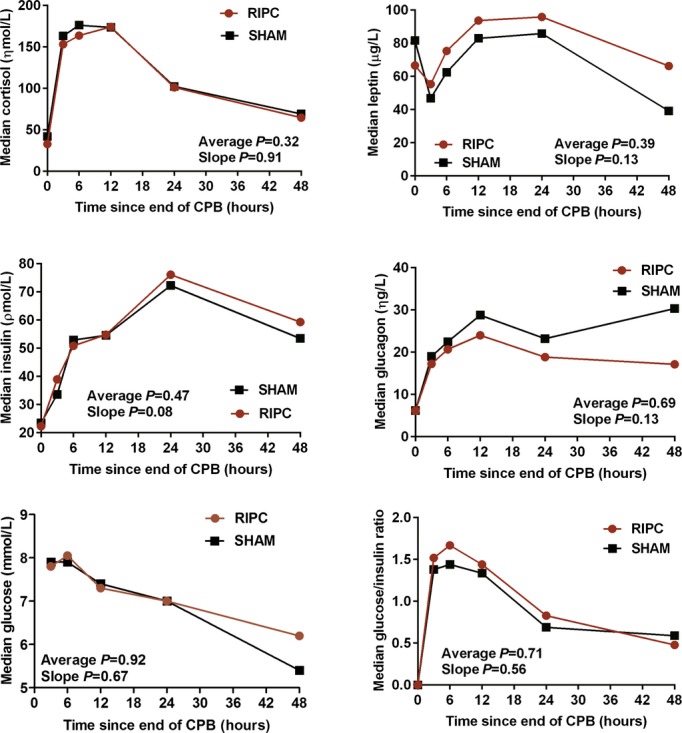
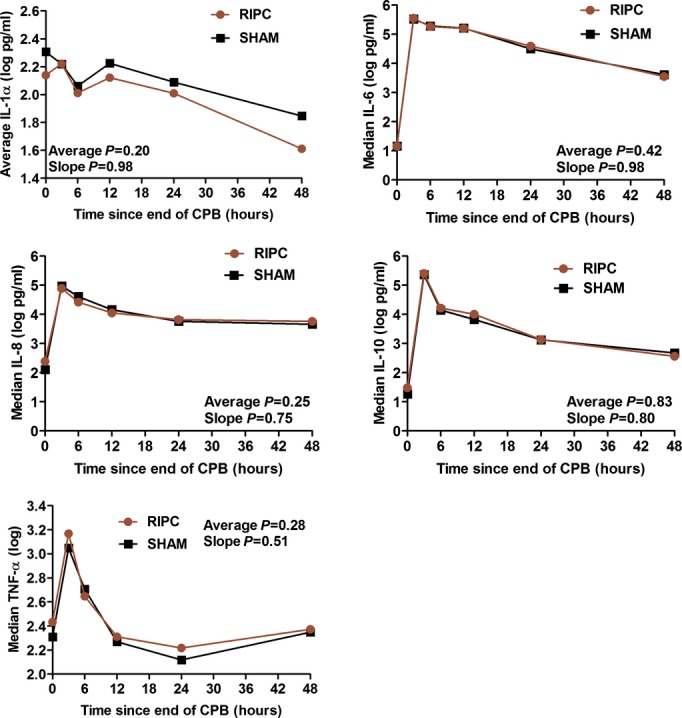
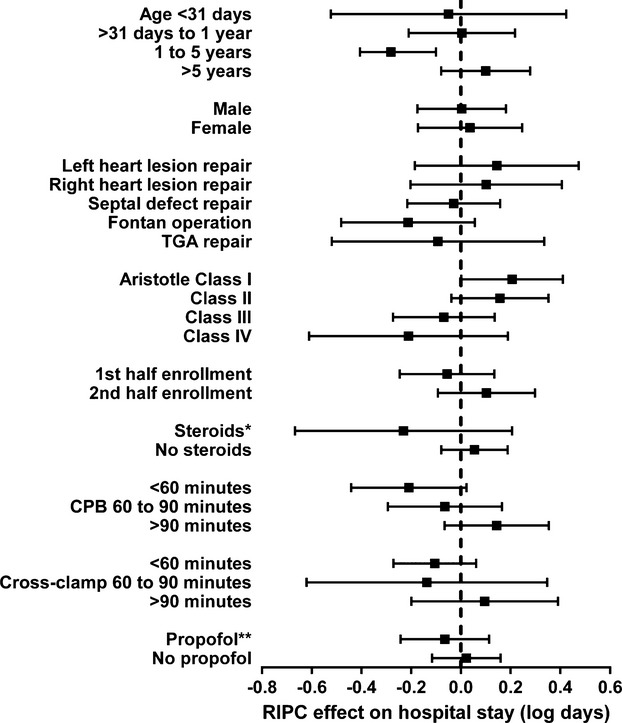
Methods and results: Overall, 299 children (aged neonate to 17 years) were randomized to receive an RIPC stimulus (inflation of a blood pressure cuff on the left thigh to 15 mm Hg above systolic for four 5-minute intervals) versus a blinded sham stimulus during induction with a standardized anesthesia protocol. Primary outcome was duration of postoperative hospital stay, with serial clinical and laboratory measurements for the first 48 postoperative hours and clinical follow-up to discharge. There were no significant baseline differences between RIPC (n=148) and sham (n=151). There were no in-hospital deaths. No significant difference in length of postoperative hospital stay was noted (sham 5.4 versus RIPC 5.6 days; difference +0.2; adjusted P=0.91), with the 95% confidence interval (-0.7 to +0.9) excluding a prespecified minimal clinically significant differences of 1 or 1.5 days. There were few significant differences in other clinical outcomes or values at time points or trends in physiological markers. Benefit was not observed in specific subgroups when explored through interactions with categories of age, sex, surgery type, Aristotle score, or first versus second half of recruitment. Adverse events were similar (sham 5%, RIPC 6%; P=0.68).
Conclusions: RIPC is not associated with important improvements in clinical outcomes and physiological markers after cardiac surgery in children.
Clinical trial registration url: clinicaltrials.gov. Unique identifier: NCT00650507.
Keywords: congenital; heart defects; pediatrics; remote ischemic preconditioning; surgery.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Levy JH, Tanaka KA. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg. 2003; 75:S715-S720. - PubMed
-
- Ungerleider RM. Optimizing response of the neonate and infant to cardiopulmonary bypass. Cardiol Young. 2005; 15suppl 1:142-148. - PubMed
-
- Hausenloy DJ, Yellon DM. The therapeutic potential of ischemic conditioning: an update. Nat Rev Cardiol. 2011; 8:619-629. - PubMed
-
- Kharbanda RK, Mortensen UM, White P, Kristiansen SB, Schmidt MR, Hoschtitzky JA, Vogel M, Sorensen K, Redington AN, MacAllister R. Transient limb ischemia induces remote ischemic preconditioning in vivo. Circulation. 2002; 106:2881-2883. - PubMed
-
- Saxena P, Newman MA, Shehatha JS, Redington AN, Konstantinov IE. Remote ischemic conditioning: evolution of the concept, mechanisms, and clinical application. J Card Surg. 2010; 25:127-134. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
