

Review
Diagnostic Lumbar Puncture
Ulster Med J.
2014 May.
Abstract
Diagnostic Lumbar Puncture is one of the most commonly performed invasive tests in clinical medicine. Evaluation of an acute headache and investigation of inflammatory or infectious disease of the nervous system are the most common indications. Serious complications are rare, and correct technique will minimise diagnostic error and maximise patient comfort. We review the technique of diagnostic Lumbar Puncture including anatomy, needle selection, needle insertion, measurement of opening pressure, Cerebrospinal Fluid (CSF) specimen handling and after care. We also make some quality improvement suggestions for those designing services incorporating diagnostic Lumbar Puncture.
Figures
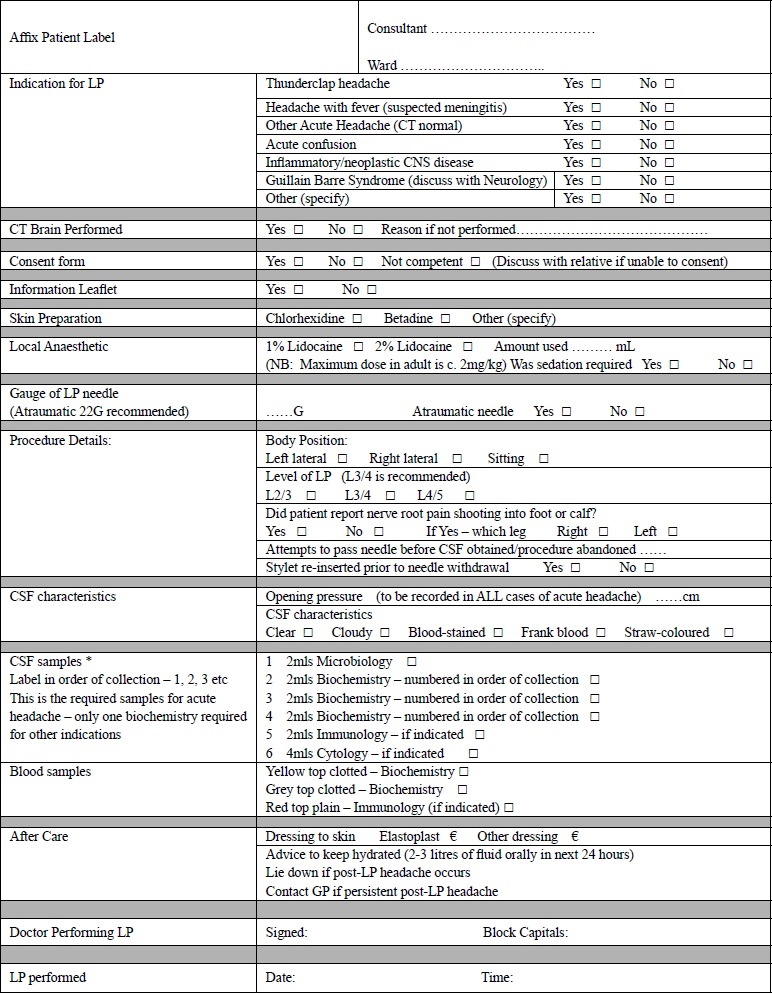
The lumbar puncture proforma currently in use in Craigavon Area Hospital
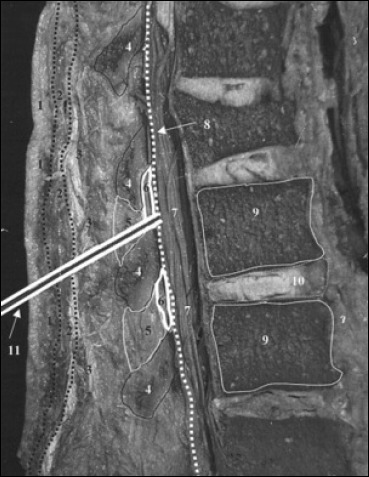
Cadaveric sagittal section through lumbar spine showing proper needle trajectory (from Boon et al.9) Sagittal section of lumbar vertebrae illustrating the course of the lumbar puncture needle through skin (1), subcutaneous tissue (2), supraspinous ligament (3), interspinous ligament (5) between the spinous processes (4), ligamentum flavum (6), dura mater (8), into the subarachnoid space and between the nerve roots of the cauda equina (7). Lumbar vertebral bodies (9), intervertebral disc (10), and lumbar puncture needle (11).
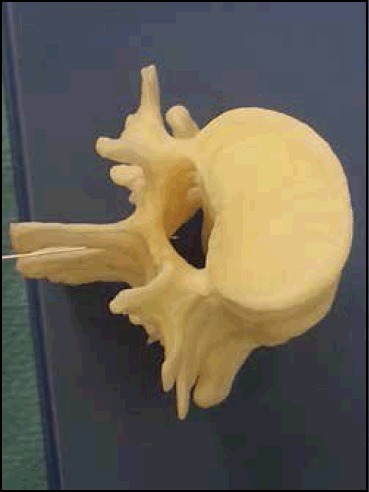
Correct position of tip of Lumbar Puncture needle in centre of Lumbar Spinal Canal at L3/4 level.
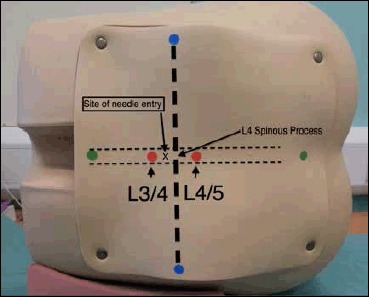
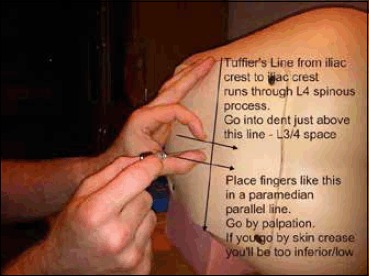
Surface Markings for Lumbar Puncture from Training Mannequin Blue dots-Iliac crests, and the line connecting them is the Intercristal Line (eponymously Tuffier's Line). Red Dots are either side of the palpated L4 spinous process, the right hand one is in the L4/5 interspinal space and the left hand one in the L3/4 interspinal space. A diagnostic Lumbar Puncture should be performed at the L3/4 interspinal space, marked ‘x’.
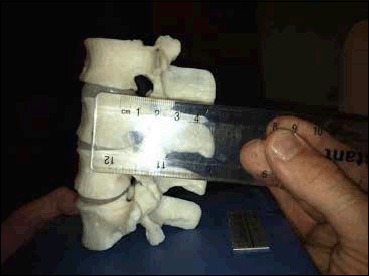
The distance from surface to Ligamentum Flavum is approximately 55mm.
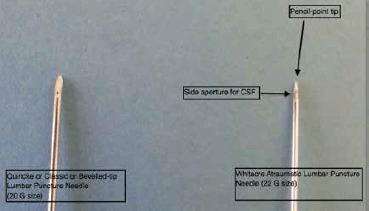
Classic (Quincke, or Bevelled-tip) and Whitacre Atraumatic Lumbar Puncture Needle
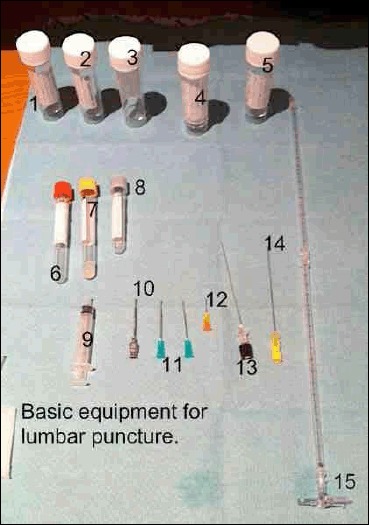
Equipment needed for Lumbar Puncture 1-5 CSF Specimen Bottles 6-7 Serum Specimen Bottles, 8 Serum glucose bottle (fluoride oxalate) 9 Syringe for local anaesthetic 10 Introducer for spinal needle (not always required) 11-12 19G and 25G hypodermic needles to draw up and inject anaesthetic 13 Whitacre 22G spinal needle (atraumatic needle) 14 Quincke 20G spinal needle (no longer recommended) 15 Manometer with 3-way tap

Three way tap attached to end of Manometer

An intradermal bleb of 0.5ml of 1% lidocaine will produce almost immediate cutaneous anaesthesia
Insertion of needle at an angle to allow passage between spinous processes of L3 and L4-note anatomical landmarks.
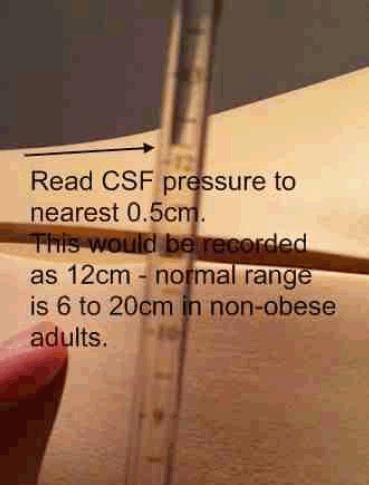
Reading CSF pressure from the top of the CSF fluid column
References
-
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before lumbar puncture in adults with suspected meningitis. N Engl J Med. 2001;345(24):1727–33. - PubMed
-
- Leeds: HSCIC. Health and Social Care Information Centre; 2012. Hospital Episode Statistics, Admitted Patient Care-England, 2011-12.
-
- Ragauskas A, Matijosaitis V, Zakelis R, Petrikonis K, Rastenyte D, Piper I, et al. Clinical assessment of noninvasive intracranial pressure absolute value measurement method. Neurology. 2012;78(21):1684–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical