

Case Report and Review of Literature: Late Retrograde Type A Aortic Dissection With Rupture after Repair of Type B Aortic Dissection with a GORE TAG Endovascular Prosthesis
- PMID: 25075169
- PMCID: PMC4082457
- DOI: 10.1055/s-0034-1373735
Case Report and Review of Literature: Late Retrograde Type A Aortic Dissection With Rupture after Repair of Type B Aortic Dissection with a GORE TAG Endovascular Prosthesis
Abstract
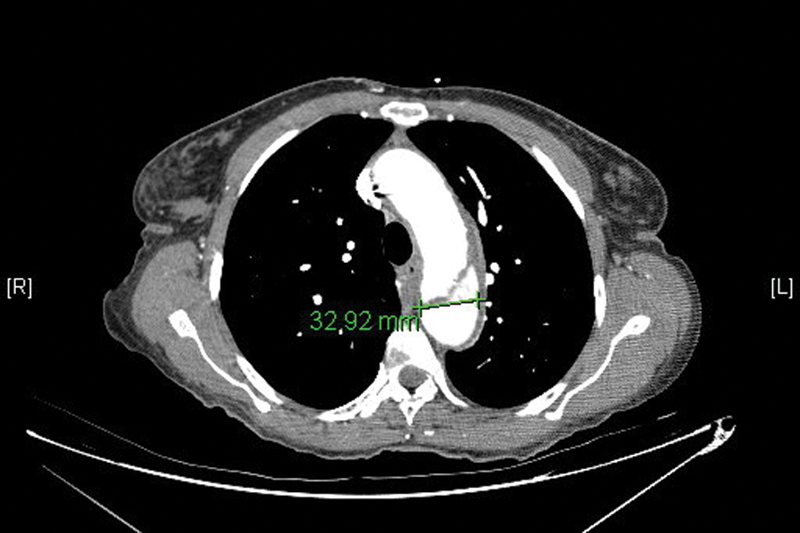
Acute aortic dissection is the most common catastrophic condition of the aorta. Treatment options include open surgery and thoracic endovascular aortic reconstruction (TEVAR). We present a late Type A dissection as a complication of the management of descending aortic dissections with TEVAR and a review of the literature. TEVAR of the thoracic aorta is a viable treatment option for the management of complicated descending thoracic aortic dissections. Careful patient selection is necessary as medical therapy successfully treats the majority of uncomplicated Type B dissections. TEVAR should be reserved for patients with complicated Type B dissections or those who fail nonoperative management. Close postoperative monitoring is necessary when TEVAR is performed and should be accompanied by lifelong surveillance. A high level of suspicion is important to identify retrograde Type A dissections in these patients given its rarity and the ambiguity of its clinical presentation.
Keywords: aortic dissection; endograft placement; endograft repair; percutaneous; risk factors; stent.
Conflict of interest statement
Figures





References
-
- LeMaire S A Green S Y Sharma K et al.Aortic root replacement with stentless porcine xenografts: early and late outcomes in 132 patients Ann Thorac Surg 2009872503–512., discussion 512–513 - PubMed
-
- Clouse W D, Hallett J W Jr, Schaff H V. et al.Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc. 2004;79(2):176–180. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
