

Saliva and plasma quantitative polymerase chain reaction-based detection and surveillance of human papillomavirus-related head and neck cancer
- PMID: 25078109
- PMCID: PMC4313904
- DOI: 10.1001/jamaoto.2014.1338
Saliva and plasma quantitative polymerase chain reaction-based detection and surveillance of human papillomavirus-related head and neck cancer
Abstract
Importance: Human papillomavirus type 16 (HPV-16) is a major causative factor in oropharyngeal squamous cell carcinoma (OPSCC). The detection of primary OPSCC is often delayed owing to the challenging anatomy of the oropharynx.
Objective: To investigate the feasibility of HPV-16 DNA detection in pretreatment and posttreatment plasma and saliva and its potential role as a marker of prognosis.
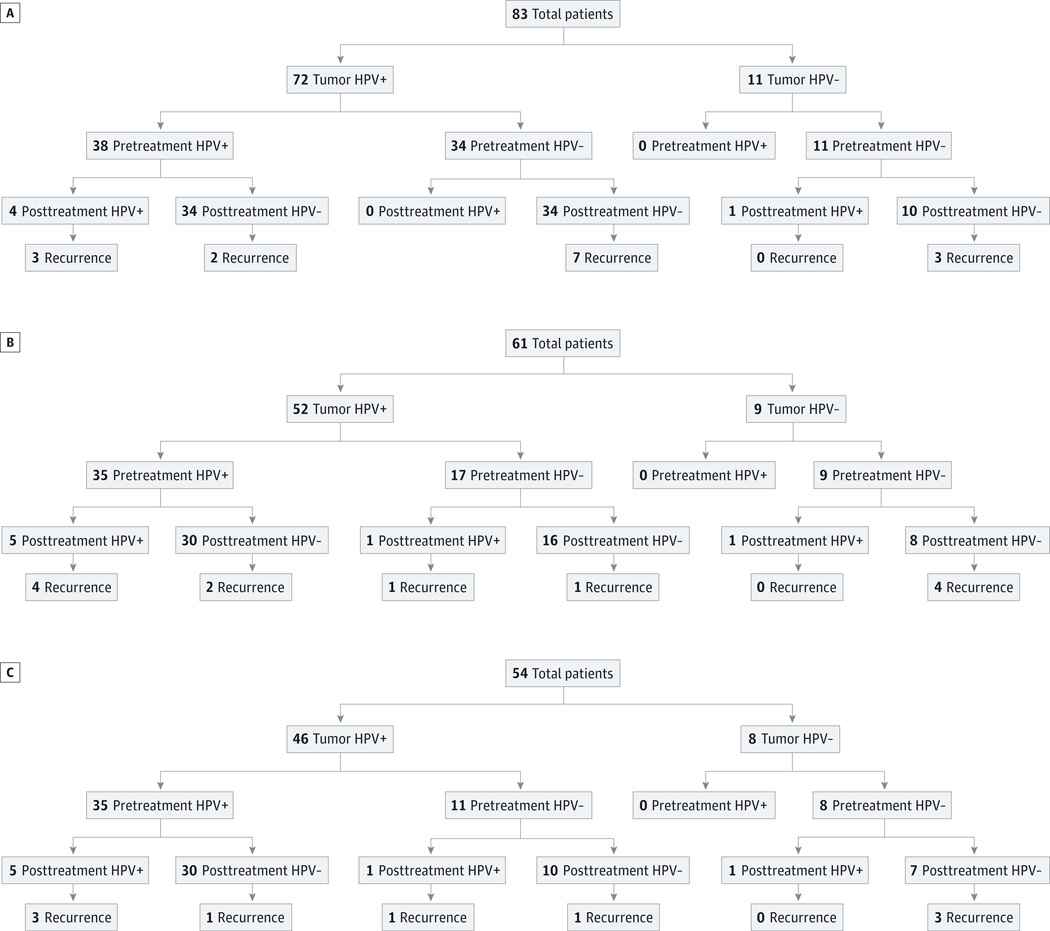
Design, setting, and participants: This is a retrospective analysis of a prospectively collected cohort. Among a cohort of patients with oropharyngeal and unknown primary squamous cell carcinoma with known HPV-16 tumor status from the Johns Hopkins Medical Institutions and Greater Baltimore Medical Center (from 1999 through 2010), 93 patients were identified with a complete set of pretreatment and posttreatment plasma or saliva samples, of which 81 patients had HPV-16-positive tumors and 12 patients had HPV-16-negative tumors. Real-time quantitative polymerase chain reaction was used to detect HPV-16 E6 and E7 DNA in saliva and plasma samples.
Main outcomes and measures: Main outcomes included sensitivity, specificity, negative predictive value of combined saliva and plasma pretreatment HPV-16 DNA status for detecting tumor HPV-16 status, as well as the association of posttreatment HPV DNA status with clinical outcomes, including recurrence-free survival and overall survival.
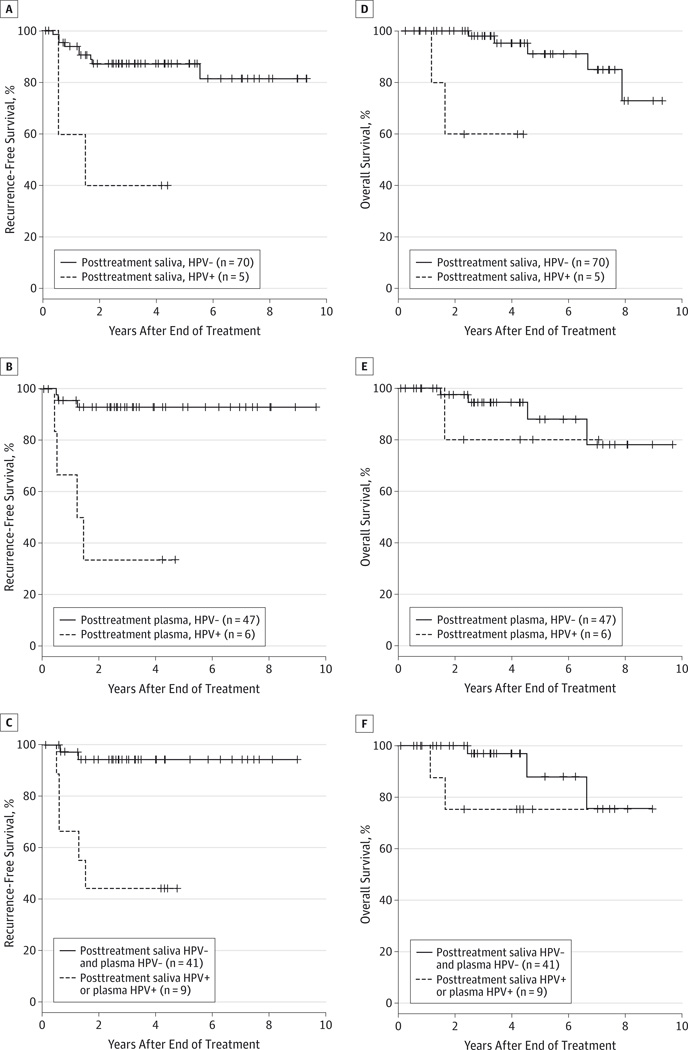
Results: The median follow-up time was 49 months (range, 0.9-181.0 months). The sensitivity, specificity, negative predictive value, and positive predictive value of combined saliva and plasma pretreatment HPV-16 DNA status for detecting tumor HPV-16 status were 76%, 100%, 42%, and 100%, respectively. The sensitivities of pretreatment saliva or plasma alone were 52.8% and 67.3%, respectively. In a multivariable analysis, positive posttreatment saliva HPV status was associated with higher risk of recurrence (hazard ratio [HR], 10.7; 95% CI, 2.36-48.50) (P = .002). Overall survival was reduced among those with posttreatment HPV-positive status in saliva (HR, 25.9; 95% CI, 3.23-208.00) (P = .002) and those with HPV-positive status in either saliva or plasma but not among patients with HPV-positive status in plasma alone. The combined saliva and plasma posttreatment HPV-16 DNA status was 90.7% specific and 69.5% sensitive in predicting recurrence within 3 years.
Conclusions and relevance: Using a combination of pretreatment plasma and saliva can increase the sensitivity of pretreatment HPV-16 status as a tool for screening patients with HPV-16-positive OPSCC. In addition, analysis of HPV-16 DNA in saliva and plasma after primary treatment may allow for early detection of recurrence in patients with HPV-16-positive OPSCC.
Conflict of interest statement
Figures
References
-
- Licitra L, Perrone F, Bossi P, et al. High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J Clin Oncol. 2006;24(36):5630–5636. - PubMed
-
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100(4):261–269. - PubMed
-
- Gillison ML. HPV and prognosis for patients with oropharynx cancer. Eur J Cancer. 2009;45(suppl 1):383–385. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
