

Endotracheal aspirate and bronchoalveolar lavage fluid analysis: interchangeable diagnostic modalities in suspected ventilator-associated pneumonia?
- PMID: 25078907
- PMCID: PMC4187781
- DOI: 10.1128/JCM.01494-14
Endotracheal aspirate and bronchoalveolar lavage fluid analysis: interchangeable diagnostic modalities in suspected ventilator-associated pneumonia?
Abstract
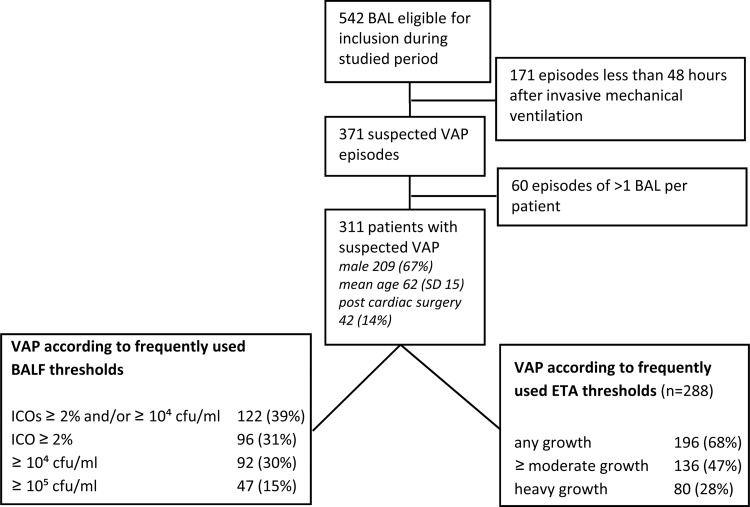
Authoritative guidelines state that the diagnosis of ventilator-associated pneumonia (VAP) can be established using either endotracheal aspirate (ETA) or bronchoalveolar lavage fluid (BALF) analysis, thereby suggesting that their results are considered to be in accordance. Therefore, the results of ETA Gram staining and semiquantitative cultures were compared to the results from a paired ETA-BALF analysis. Different thresholds for the positivity of ETAs were assessed. This was a prospective study of all patients who underwent bronchoalveolar lavage for suspected VAP in a 27-bed university intensive care unit during an 8-year period. VAP was diagnosed when ≥ 2% of the BALF cells contained intracellular organisms and/or when BALF quantitative culture revealed ≥ 10(4) CFU/ml of potentially pathogenic microorganisms. ETA Gram staining and semiquantitative cultures were compared to the results from paired BALF analysis by Cohen's kappa coefficients. VAP was suspected in 311 patients and diagnosed in 122 (39%) patients. In 288 (93%) patients, the results from the ETA analysis were available for comparison. Depending on the threshold used and the diagnostic modality, VAP incidences varied from 15% to 68%. For the diagnosis of VAP, the most accurate threshold for positivity of ETA semiquantitative cultures was moderate or heavy growth, whereas the optimal threshold for BALF Gram staining was ≥ 1 microorganisms per high power field. The Cohen's kappa coefficients were 0.22, 0.31, and 0.60 for ETA and paired BALF Gram stains, cultures, and BALF Gram stains, respectively. Since the ETA and BALF Gram stains and cultures agreed only fairly, they are probably not interchangeable for diagnosing VAP.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures

References
-
- Melsen WG, Rovers MM, Groenwold RH, Bergmans DC, Camus C, Bauer TT, Hanisch EW, Klarin B, Koeman M, Krueger WA, Lacherade JC, Lorente L, Memish ZA, Morrow LE, Nardi G, van Nieuwenhoven CA, O'Keefe GE, Nakos G, Scannapieco FA, Seguin P, Staudinger T, Topeli A, Ferrer M, Bonten MJ. 2013. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 13:665–671. 10.1016/S1473-3099(13)70081-1 - DOI - PubMed
-
- Luna CM, Aruj P, Niederman MS, Garzón J, Violi D, Prignoni A, Ríos F, Baquero S, Gando S, Grupo Argentino de Estudio de la Neumonía Asociada al Respirador Group 2006. Appropriateness and delay to initiate therapy in ventilator-associated pneumonia. Eur. Respir. J. 27:158–164. 10.1183/09031936.06.00049105 - DOI - PubMed
-
- Novosel TJ, Hodge LA, Weireter LJ, Britt RC, Collins JN, Reed SF, Britt LD. 2012. Ventilator-associated pneumonia: depends on your definition. Am. Surg. 78:851–854 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
