

The effect of interleukin-1 receptor antagonist therapy on markers of inflammation in non-ST elevation acute coronary syndromes: the MRC-ILA Heart Study
- PMID: 25079365
- PMCID: PMC4320321
- DOI: 10.1093/eurheartj/ehu272
The effect of interleukin-1 receptor antagonist therapy on markers of inflammation in non-ST elevation acute coronary syndromes: the MRC-ILA Heart Study
Abstract
Aims: Acute coronary syndromes (ACSs) are driven by inflammation within coronary plaque. Interleukin-1 (IL-1) has an established role in atherogenesis and the vessel-response to injury. ACS patients have raised serum markers of inflammation. We hypothesized that if IL-1 is a driving influence of inflammation in non-ST elevation ACS (NSTE-ACS), IL-1 inhibition would reduce the inflammatory response at the time of ACS.
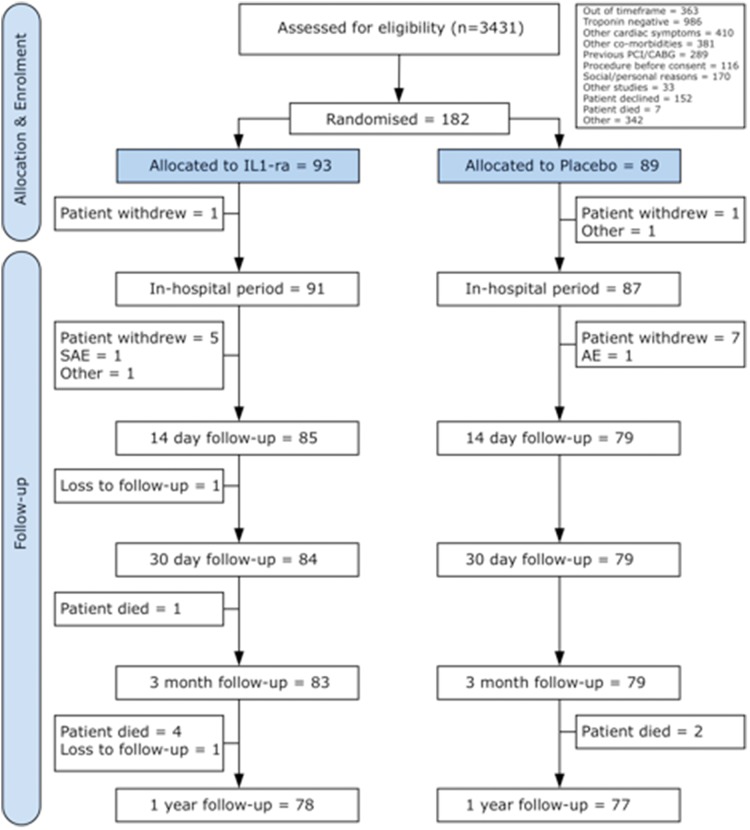
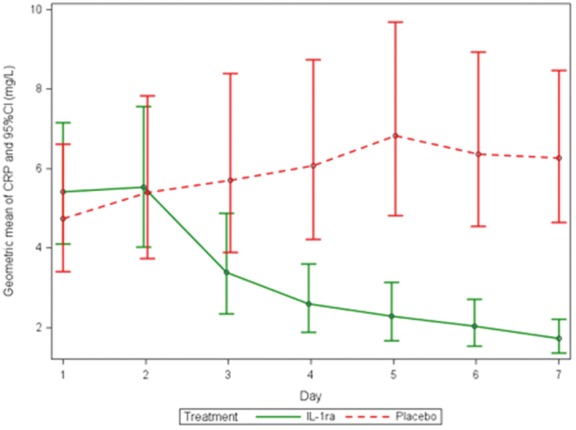
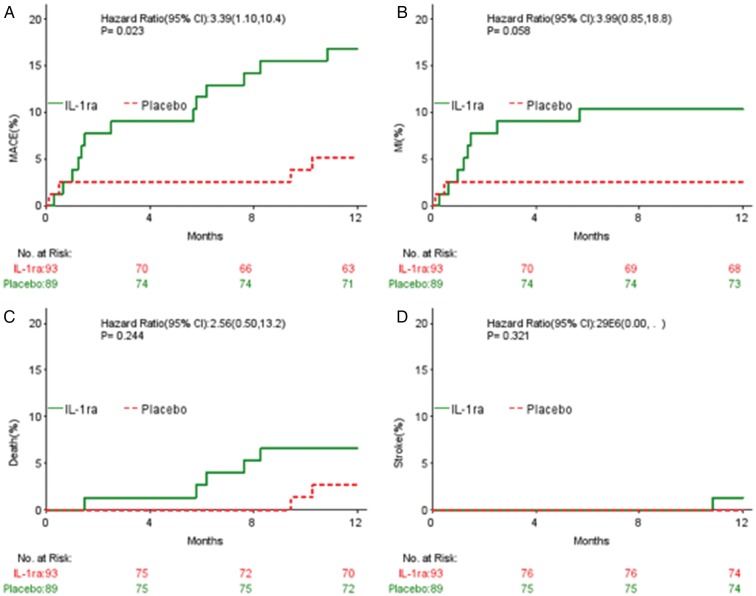
Methods and results: A phase II, double-blinded, randomized, placebo-controlled, study recruited 182 patients with NSTE-ACS, presenting <48 h from onset of chest pain. Treatment was 1:1 allocation to daily, subcutaneous IL-1receptor antagonist (IL-1ra) or placebo for 14 days. Baseline characteristics were well matched. Treatment compliance was 85% at 7 days. The primary endpoint (area-under-the-curve for C-reactive protein over the first 7 days) was: IL-1ra group, 21.98 mg day/L (95%CI 16.31-29.64); placebo group, 43.5 mg day/L (31.15-60.75) (geometric mean ratio = 0.51 mg/L; 95%CI 0.32-0.79; P = 0.0028). In the IL-1ra group, 14-day achieved high-sensitive C-reactive protein (P < 0.0001) and IL-6 levels (P = 0.02) were lower than Day 1. Sixteen days after discontinuation of treatment (Day 30) high-sensitive C-reactive protein levels had risen again in the IL-1ra group [IL-1ra; 3.50 mg/L (2.65-4.62): placebo; 2.21 mg/L (1.67-2.92), P = 0.022]. MACE at Day 30 and 3 months was similar but at 1 year there was a significant excess of events in the IL-1ra group.
Conclusion: IL-1 drives C-reactive protein elevation at the time of NSTE-ACS. Following 14 days IL-1ra treatment inflammatory markers were reduced. These results show the importance of IL-1 as a target in ACS, but also indicate the need for additional studies with anti-IL-1 therapy in ACS to assess duration and safety.
Clinical trial registration euctr: 2006-001767-31-GB: www.clinicaltrialsregister.eu/ctr-search/trial/2006-001767-31/GB.
Keywords: Drugs; Interleukins; Myocardial infarction.
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Anti-inflammatory therapies in acute coronary syndromes: is IL-1 blockade a solution?Eur Heart J. 2015 Feb 7;36(6):337-9. doi: 10.1093/eurheartj/ehu369. Epub 2014 Sep 8. Eur Heart J. 2015. PMID: 25205529 No abstract available.
References
-
- Libby P. Mechanisms of acute coronary syndromes and their implications for therapy. N Engl J Med. 2013;368:2004–2013. - PubMed
-
- Ross R. Atherosclerosis – an inflammatory disease. N Engl J Med. 1999;340:115–126. - PubMed
-
- Glass CK, Witztum JL. Atherosclerosis: the road ahead review. Cell. 2001;104:503–516. - PubMed
-
- Galea J, Armstrong J, Gadsdon P, Holden H, Francis SE, Holt CM. Interleukin-1 beta in coronary arteries of patients with ischemic heart disease. Arterioscler Thromb Vasc Biol. 1996;16:1000–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
