

A pharmacokinetic model of a tissue implantable insulin sensor
- PMID: 25080048
- PMCID: PMC6438194
- DOI: 10.1002/adhm.201400264
A pharmacokinetic model of a tissue implantable insulin sensor
Abstract
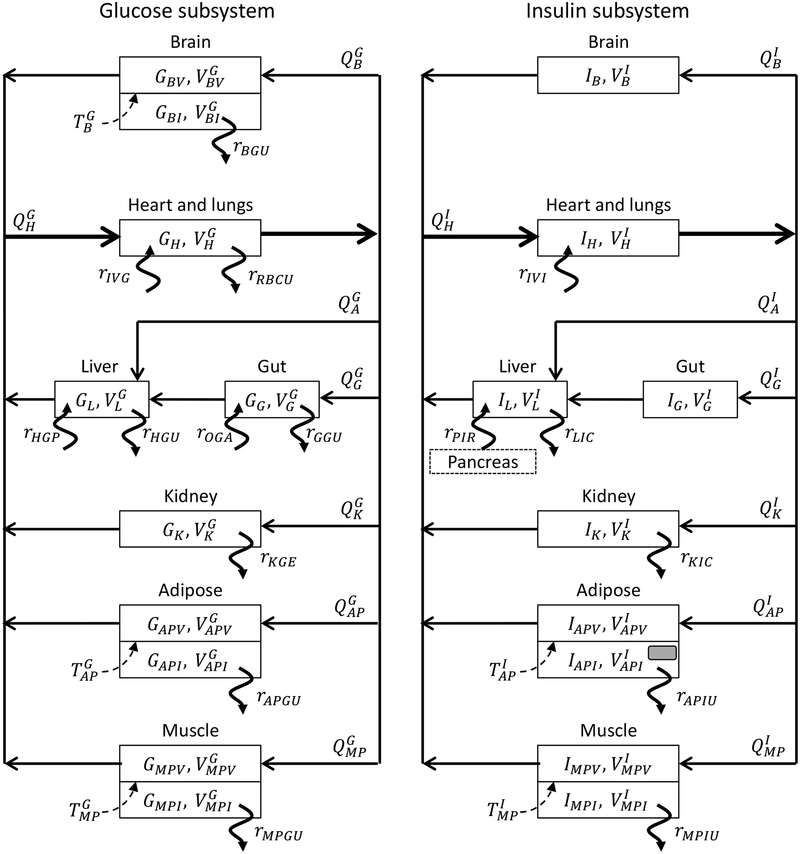
While implantable sensors such as the continuous glucose monitoring system have been widely studied, both experimentally and mathematically, relatively little attention has been applied to the potential of insulin sensors. Such sensors can provide feedback control for insulin infusion systems and pumps and provide platforms for the monitoring of other biomarkers in vivo. In this work, the first pharmacokinetic model of an affinity sensor is developed for insulin operating subcutaneously in the limit of where mass transfer across biological membranes reaches a steady state. Using a physiological, compartmental model for glucose, insulin, and glucagon metabolism, the maximum sensor response and its delay time relative to plasma insulin concentration, are calculated based on sensor geometry, placement, and insulin binding parameters for a sensor localized within adipose tissue. A design relation is derived linking sensor dynamics to insulin time lag and placement within human tissue. The model should find utility in understanding dynamic insulin responses and forms the basis of model predictive control algorithms that incorporate sensor dynamics.
Keywords: insulin sensors; single-walled carbon nanotubes.
© 2014 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Figures






References
-
- Bascones-Martinez A, Matesanz-Perez P, Escribano-Bermejo M, Gonzalez-Moles MA, Bascones-Ilundain J, Meurman JH, Med Oral Patol Oral Cir Bucal 2011, 16, e722–729. - PubMed
-
- Bergenstal RM, Tamborlane WV, Ahmann A, Buse JB, Dailey G, Davis SN, Joyce C, Peoples T, Perkins BA, Welsh JB, Willi SM, Wood MA, New England Journal of Medicine 2010, 363, 311–320. - PubMed
-
- Bennett CM, Guo M, Dharmage SC, Diabetic Medicine 2007, 24, 333–343. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
