

Cross-sectional study of 168 patients with hepatorenal tyrosinaemia and implications for clinical practice
- PMID: 25081276
- PMCID: PMC4347563
- DOI: 10.1186/s13023-014-0107-7
Cross-sectional study of 168 patients with hepatorenal tyrosinaemia and implications for clinical practice
Abstract
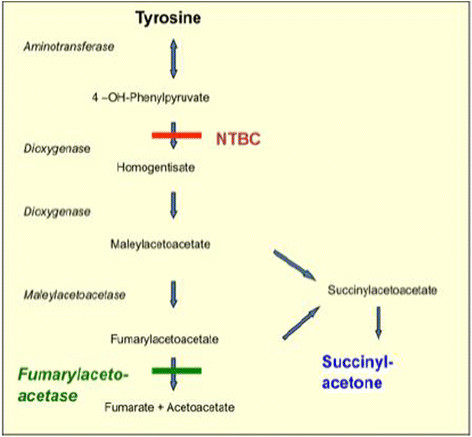
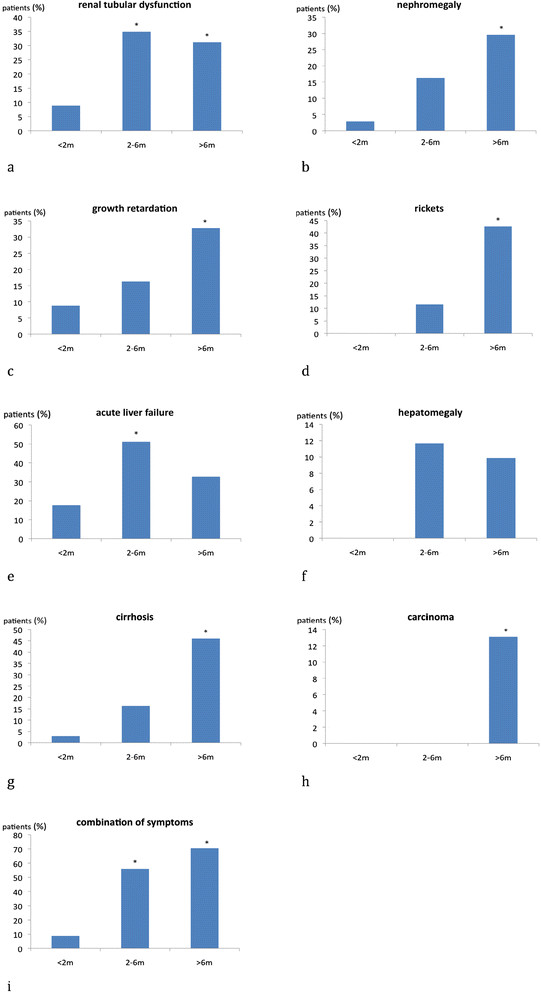
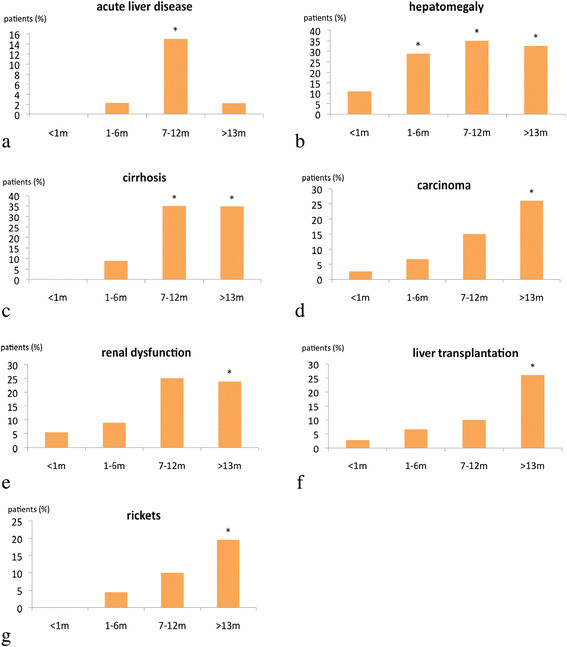
Background: Hepatorenal tyrosinaemia (Tyr 1) is a rare inborn error of tyrosine metabolism. Without treatment, patients are at high risk of developing acute liver failure, renal dysfunction and in the long run hepatocellular carcinoma. The aim of our study was to collect cross-sectional data.
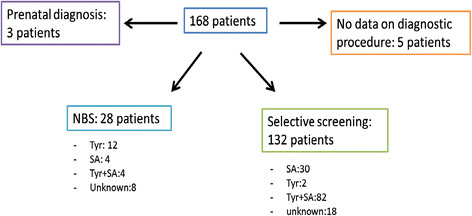
Methods: Via questionnaires we collected retrospective data of 168 patients with Tyr 1 from 21 centres (Europe, Turkey and Israel) about diagnosis, treatment, monitoring and outcome. In a subsequent consensus workshop, we discussed data and clinical implications.
Results: Early treatment by NTBC accompanied by diet is essential to prevent serious complications such as liver failure, hepatocellular carcinoma and renal disease. As patients may remain initially asymptomatic or develop uncharacteristic clinical symptoms in the first months of life newborn mass screening using succinylacetone (SA) as a screening parameter in dried blood is mandatory for early diagnosis. NTBC-treatment has to be combined with natural protein restriction supplemented with essential amino acids. NTBC dosage should be reduced to the minimal dose allowing metabolic control, once daily dosing may be an option in older children and adults in order to increase compliance. Metabolic control is judged by SA (below detection limit) in dried blood or urine, plasma tyrosine (<400 μM) and NTBC-levels in the therapeutic range (20-40 μM). Side effects of NTBC are mild and often transient. Indications for liver transplantation are hepatocellular carcinoma or failure to respond to NTBC. Follow-up procedures should include liver and kidney function tests, tumor markers and imaging, ophthalmological examination, blood count, psychomotor and intelligence testing as well as therapeutic monitoring (SA, tyrosine, NTBC in blood).
Conclusion: Based on the data from 21 centres treating 168 patients we were able to characterize current practice and clinical experience in Tyr 1. This information could form the basis for clinical practice recommendations, however further prospective data are required to underpin some of the recommendations.
Figures
References
-
- Chakrapani A, Holme E. In: Inborn Metabolic diseases. 4. Fernandez S, Berghe W, editor. Springer, Heidelberg; 2006. Disorders of tyrosine metabolism; pp. 233–243.
-
- Van Spronsen FJ, Bijleveld MA, van Maldegem BT, Wijburg FA. Hepatocellular Carcinoma in Hereditary Tyrosinemia Type I Despite 2-(2 Nitro-4-3-Trifluoro-Methylbenzoyl)-1,3-Cyclohexanedione Treatment. J Pedriatr Gastroenterol Nutr. 2005;40:90–93. - PubMed
-
- Weinberg AG, Mize CE, Worthen HG. The occurence of hepatoma in the chronic form of hereditary tyrosinemia. J Pediatr. 1976;88:434–438. - PubMed
-
- Thimm E, Richter-Werkle R, Kamp G, Molke B, Herebian D, Klee D, Mayatepek E, Spiekerkoetter U. Neurocognitive outcome in patients with hypertyrosinemia type I after a long-term treatment with NTBC. J Inherit Metab Dis. 2012;35:263–268. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
