

Giant, completely calcified lumbar juxtafacet cyst: report of an unusual case
- PMID: 25083359
- PMCID: PMC4111943
- DOI: 10.1055/s-0033-1363591
Giant, completely calcified lumbar juxtafacet cyst: report of an unusual case
Abstract
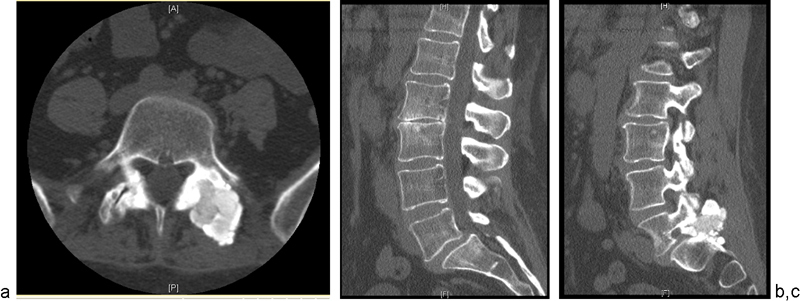
Study Design Case report. Objective To report the case of one patient who developed a giant, completely calcified, juxtafacet cyst. Methods A 57-year-old woman presented with a 2-year history of progressively worsening lower back pain, left leg pain, weakness, and paresthesias. Imaging showed a giant, completely calcified mass arising from the left L5-S1 facet joint, with coexisting grade I L5 on S1 anterolisthesis. The patient was treated with laminectomy, excision of the mass, and L5-S1 fixation and fusion. Results The patient had an uncomplicated postoperative course and had complete resolution of her symptoms as of 1-year follow-up. Conclusions When presented with a solid-appearing, calcified mass arising from the facet joint, a completely calcified juxtafacet cyst should be considered as part of the differential diagnosis.
Keywords: case report; complete calcification; juxtafacet cyst; synovial cyst.
Conflict of interest statement
Figures




References
-
- Onofrio B M, Mih A D. Synovial cysts of the spine. Neurosurgery. 1988;22(4):642–647. - PubMed
-
- Salmon B, Martin D, Lenelle J, Stevenaert A. Juxtafacet cyst of the lumbar spine. Clinical, radiological and therapeutic aspects in 28 cases. Acta Neurochir (Wien) 2001;143(2):129–134. - PubMed
-
- Banning C S, Thorell W E, Leibrock L G. Patient outcome after resection of lumbar juxtafacet cysts. Spine (Phila Pa 1976) 2001;26(8):969–972. - PubMed
-
- Sabo R A, Tracy P T, Weinger J M. A series of 60 juxtafacet cysts: clinical presentation, the role of spinal instability, and treatment. J Neurosurg. 1996;85(4):560–565. - PubMed
-
- Xu R, McGirt M J, Parker S L. et al.Factors associated with recurrent back pain and cyst recurrence after surgical resection of one hundred ninety-five spinal synovial cysts: analysis of one hundred sixty-seven consecutive cases. Spine (Phila Pa 1976) 2010;35(10):1044–1053. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
