

Resection of Primary Brachial Plexus Tumor via a Modified Supraclavicular Approach
- PMID: 25083372
- PMCID: PMC4110154
- DOI: 10.1055/s-0034-1376423
Resection of Primary Brachial Plexus Tumor via a Modified Supraclavicular Approach
Abstract
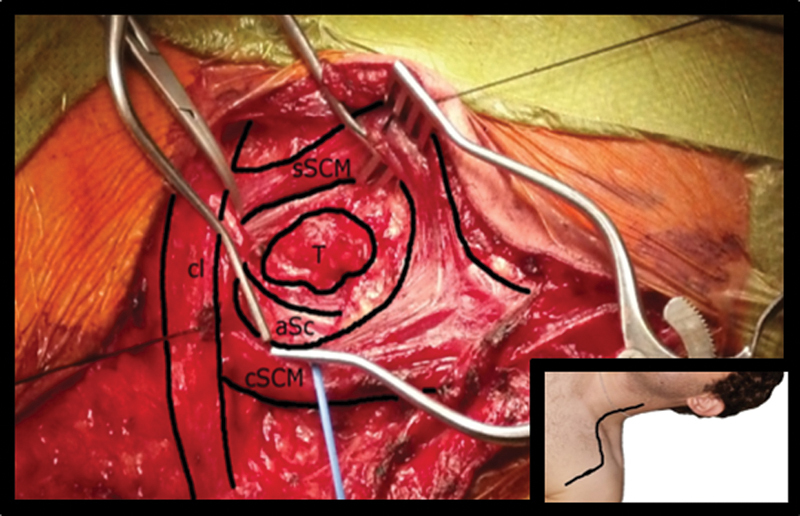
Benign peripheral nerve sheath tumors are generally considered curable lesions, and surgical resection is recommended as the primary line of treatment. When these tumors occur in the brachial plexus, they are most frequently accessed via the supraclavicular approach. Traditional descriptions of this approach have included either transection of sternocleidomastoid (SCM) muscle fibers or disarticulation of the clavicular head of the SCM muscle. This report presents a simple and easy-to-adapt modification of the supraclavicular approach that offers greater preservation of the SCM muscle. The modification primarily consists of the creation of an intramuscular window between the sternal and clavicular heads of the SCM via the splitting and dilation SCM muscle fibers. This technique minimizes the disruption of SCM muscle tissue compared with previous descriptions and may be associated with improved postoperative pain and return to function.
Keywords: brachial plexus tumor; intramuscular window; sternocleidomastoid muscle; supraclavicular approach.
Figures

References
-
- Huang J H, Zaghloul K, Zager E L. Surgical management of brachial plexus region tumors. Surg Neurol. 2004;61(4):372–378. - PubMed
-
- Tender G C Kline D G Anterior supraclavicular approach to the brachial plexus Neurosurgery 2006584, Suppl 02ONS-360–ONS-364; discussion ONS-364–ONS-365 - PubMed
-
- Tender G C Kline D G The infraclavicular approach to the brachial plexus Neurosurgery 2008623, Suppl 01180–184.; discussion 184–185 - PubMed
-
- Zadnik M, Eglseder W A Jr, Shur V B. Transclavicular approach for brachial plexus reconstruction. Tech Hand Up Extrem Surg. 2008;12(2):126–130. - PubMed
-
- Thatte M R, Agashe M, Rathod C, Lad P, Mehta R. An approach to the supraclavicular and infraclavicular aspects of the brachial plexus. Tech Hand Up Extrem Surg. 2011;15(3):188–197. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources