

Endoscopy-assisted breast-conserving surgery for breast cancer patients
- PMID: 25083503
- PMCID: PMC4115765
- DOI: 10.3978/j.issn.2227-684X.2013.12.04
Endoscopy-assisted breast-conserving surgery for breast cancer patients
Abstract
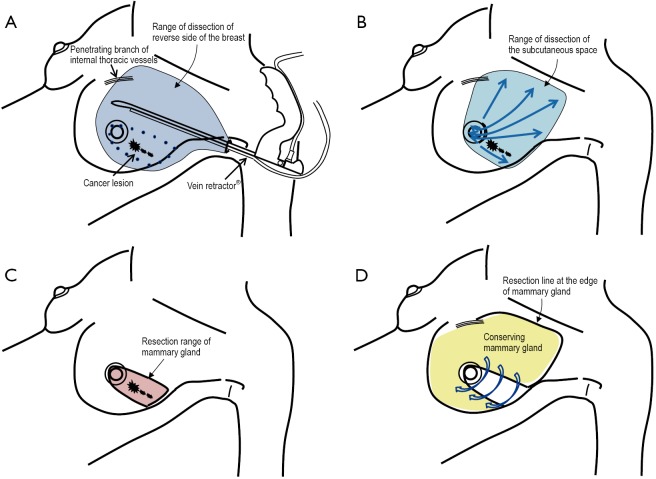
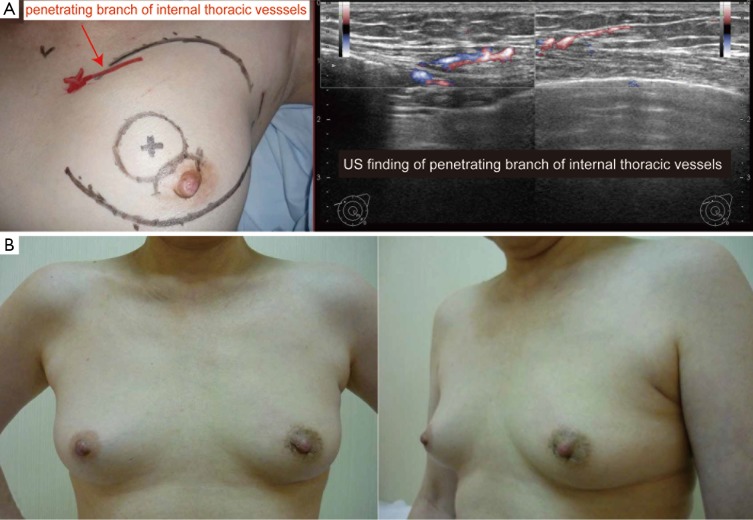
Breast-conserving surgery (BCS) combined with postoperative radiotherapy is a standard therapy for early-stage breast cancer patients. In addition, recent developments in oncoplastic surgery have improved cosmetic outcomes and patient satisfaction. Therefore, a breast surgeon's current role in BCS is not only to perform a curative resection of cancerous lesions with adequate surgical margins, but also to preserve the shape and appearance of the treated breast. Endoscopy-assisted breast-conserving surgery (EBCS), which has the advantage of a less noticeable scar, was developed more than ten years ago. Recently, some clinical studies have reported the feasibility, oncological outcomes, aesthetic outcomes, and patient satisfaction of EBCS. Herein, we will review the EBCS clinical studies that have been conducted so far and discuss current issues regarding this operative method.
Keywords: Endoscopy assisted; breast cancer; breast surgery; breast-conserving surgery (BCS); endoscope.
Figures
Similar articles
-
Technical feasibility and cosmetic advantage of hybrid endoscopy-assisted breast-conserving surgery for breast cancer patients.J Laparoendosc Adv Surg Tech A. 2013 Feb;23(2):91-9. doi: 10.1089/lap.2012.0224. Epub 2012 Dec 28. J Laparoendosc Adv Surg Tech A. 2013. PMID: 23272727
-
Endoscopic assisted breast conserving surgery for breast cancer: Clinical outcome, learning curve, and patient reported aesthetic results from preliminary 100 procedures.Eur J Surg Oncol. 2020 Aug;46(8):1446-1455. doi: 10.1016/j.ejso.2020.02.020. Epub 2020 Feb 20. Eur J Surg Oncol. 2020. PMID: 32115333
-
Endoscopy-assisted breast-conserving surgery for early breast cancer.Asian J Endosc Surg. 2013 Aug;6(3):203-8. doi: 10.1111/ases.12018. Epub 2013 Feb 1. Asian J Endosc Surg. 2013. PMID: 23368666
-
Endoscopy-assisted breast conservation surgery (E-BCS) vs conventional breast conservation surgery (C-BCS) technique for the management of early breast cancer: A systematic review and meta-analysis.Breast Dis. 2023;42(1):383-393. doi: 10.3233/BD-230023. Breast Dis. 2023. PMID: 38108340
-
Evolution of breast conserving surgery-current implementation of oncoplastic techniques in breast conserving surgery: a literature review.Gland Surg. 2024 Mar 27;13(3):412-425. doi: 10.21037/gs-23-454. Epub 2024 Mar 14. Gland Surg. 2024. PMID: 38601289 Free PMC article. Review.
Cited by
-
Comparing outcomes of single-port insufflation endoscopic breast-conserving surgery and conventional open approach for breast cancer.World J Surg Oncol. 2022 Oct 6;20(1):335. doi: 10.1186/s12957-022-02798-6. World J Surg Oncol. 2022. PMID: 36203177 Free PMC article.
-
Single-port three-dimensional (3D) endoscopic-assisted breast surgery-preliminary results and patient-reported satisfaction in 145 breast cancer and gynecomastia cases.World J Surg Oncol. 2023 Oct 26;21(1):335. doi: 10.1186/s12957-023-03191-7. World J Surg Oncol. 2023. PMID: 37880770 Free PMC article.
-
Evolution of minimal access breast surgery.Gland Surg. 2019 Dec;8(6):784-793. doi: 10.21037/gs.2019.11.16. Gland Surg. 2019. PMID: 32042687 Free PMC article. Review.
-
Development of video-assisted breast cancer surgery: Initial experience with a novel method for creating working space without prior liposuction.Mol Clin Oncol. 2017 Jul;7(1):32-38. doi: 10.3892/mco.2017.1279. Epub 2017 May 31. Mol Clin Oncol. 2017. PMID: 28685071 Free PMC article.
-
Comparison of endoscopic breast-conserving surgery versus conventional breast-conserving surgery for the treatment of early-stage breast cancer: a meta-analysis.Front Oncol. 2024 Aug 6;14:1419123. doi: 10.3389/fonc.2024.1419123. eCollection 2024. Front Oncol. 2024. PMID: 39165683 Free PMC article.
References
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002;347:1233-41 - PubMed
-
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 2002;347:1227-32 - PubMed
-
- Litière S, Werutsky G, Fentiman IS, et al. Breast conserving therapy versus mastectomy for stage I-II breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomised trial. Lancet Oncol 2012;13:412-9 - PubMed
-
- Tamaki Y, Sakita I, Miyoshi Y, et al. Transareolar endoscopy-assisted partial mastectomy: a preliminary report of six cases. Surg Laparosc Endosc Percutan Tech 2001;11:356-62 - PubMed
-
- Owaki T, Yoshinaka H, Ehi K, et al. Endoscopic quadrantectomy for breast cancer with sentinel lymph node navigation via a small axillary incision. Breast 2005;14:57-60 - PubMed
Publication types
LinkOut - more resources
Full Text Sources