

Acute care clinical indicators associated with discharge outcomes in children with severe traumatic brain injury
- PMID: 25083982
- PMCID: PMC4167478
- DOI: 10.1097/CCM.0000000000000507
Acute care clinical indicators associated with discharge outcomes in children with severe traumatic brain injury
Abstract
Objective: The effect of the 2003 severe pediatric traumatic brain injury (TBI) guidelines on outcomes has not been examined. We aimed to develop a set of acute care guideline-influenced clinical indicators of adherence and tested the relationship between these indicators during the first 72 hours after hospital admission and discharge outcomes.
Design: Retrospective multicenter cohort study.
Setting: Five regional pediatric trauma centers affiliated with academic medical centers.
Patients: Children under 18 years with severe traumatic brain injury (admission Glasgow Coma Scale score ≤ 8, International Classification of Diseases, 9th Edition, diagnosis codes of 800.0-801.9, 803.0-804.9, 850.0-854.1, 959.01, 950.1-950.3, 995.55, maximum head abbreviated Injury Severity Score ≥ 3) who received tracheal intubation for at least 48 hours in the ICU between 2007 and 2011 were examined.
Interventions: None.
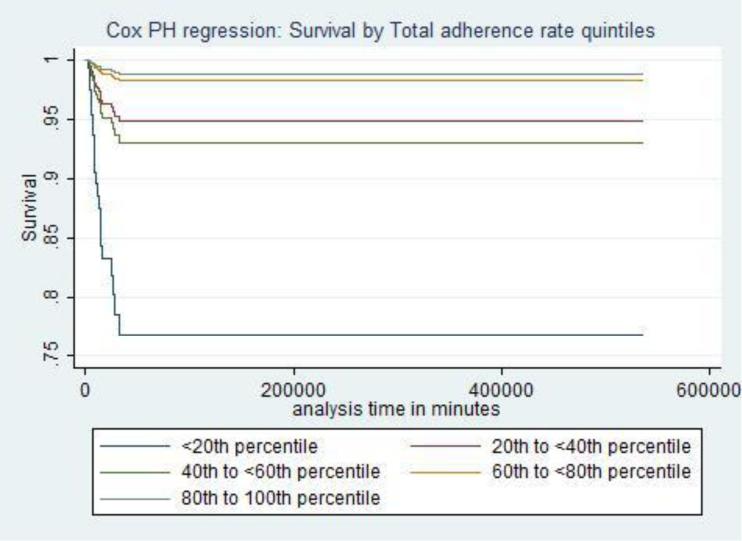
Measurements and main results: Total percent adherence to the clinical indicators across all treatment locations (prehospital, emergency department, operating room, and ICU) during the first 72 hours after admission to study center were determined. Main outcomes were discharge survival and Glasgow Outcome Scale score. Total adherence rate across all locations and all centers ranged from 68% to 78%. Clinical indicators of adherence were associated with survival (adjusted hazard ratios, 0.94; 95% CI, 0.91-0.96). Three indicators were associated with survival: absence of prehospital hypoxia (adjusted hazard ratios, 0.20; 95% CI, 0.08-0.46), early ICU start of nutrition (adjusted hazard ratios, 0.06; 95% CI, 0.01-0.26), and ICU PaCO2 more than 30 mm Hg in the absence of radiographic or clinical signs of cerebral herniation (adjusted hazard ratios, 0.22; 95% CI, 0.06-0.8). Clinical indicators of adherence were associated with favorable Glasgow Outcome Scale among survivors (adjusted hazard ratios, 0.99; 95% CI, 0.98-0.99). Three indicators were associated with favorable discharge Glasgow Outcome Scale: all operating room cerebral perfusion pressure more than 40 mm Hg (adjusted relative risk, 0.61; 95% CI, 0.58-0.64), all ICU cerebral perfusion pressure more than 40 mm Hg (adjusted relative risk, 0.73; 95% CI, 0.63-0.84), and no surgery (any type; adjusted relative risk, 0.68; 95% CI, 0.53- 0.86).
Conclusions: Acute care clinical indicators of adherence to the Pediatric Guidelines were associated with significantly higher discharge survival and improved discharge Glasgow Outcome Scale. Some indicators were protective, regardless of treatment location, suggesting the need for an interdisciplinary approach to the care of children with severe traumatic brain injury.
Figures
Comment in
-
Adherence to the guidelines for management of severe pediatric traumatic brain injury: enough evidence to support benefit?*.Crit Care Med. 2014 Oct;42(10):2308-9. doi: 10.1097/CCM.0000000000000563. Crit Care Med. 2014. PMID: 25226130 No abstract available.
References
-
- Faul M, Xu L, Wald MM, et al. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002-2006. Centers for Disease Control, National Center for Injury Prevention and Control; Atlanta, GA: 2010.
-
- Kouznetsov E, Brennan M, Vassilyadi M. Towards development of a survival prediction tool for pediatric head injury. Pediatr Neurosurg. 2012;48(1):1–5. doi: 10.1159/000340068. Epub 2012 Aug 21. - PubMed
-
- Sills MR, Libby AM, Orton HD. Prehospital and in-hospital mortality: a comparison of intentional and unintentional traumatic brain injuries in Colorado children. Arch Pediatr Adolesc Med. 2005 Jul;159(7):665–670. - PubMed
-
- Zebrack M, Dandoy C, Hansen K, Scaife E, Mann NC, Bratton SL. Early resuscitation of children with moderate-to-severe traumatic brain injury. Pediatrics. 2009 Jul;124(1):56–64. doi: 10.1542/peds.2008-1006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
