

Biology and principles of scar management and burn reconstruction
- PMID: 25085089
- PMCID: PMC4286257
- DOI: 10.1016/j.suc.2014.05.005
Biology and principles of scar management and burn reconstruction
Abstract
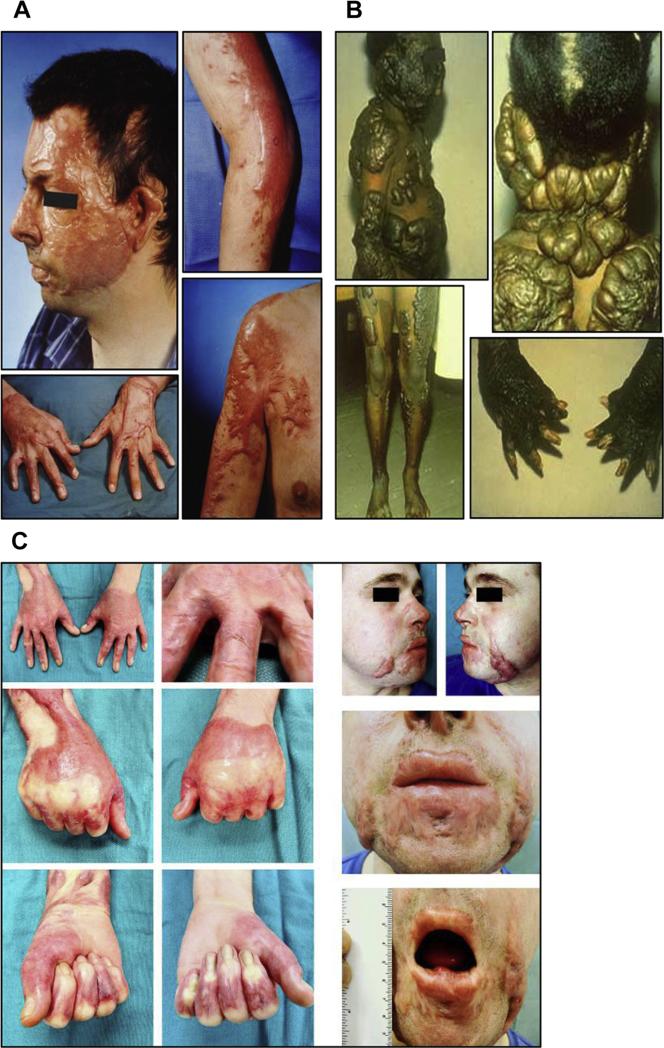
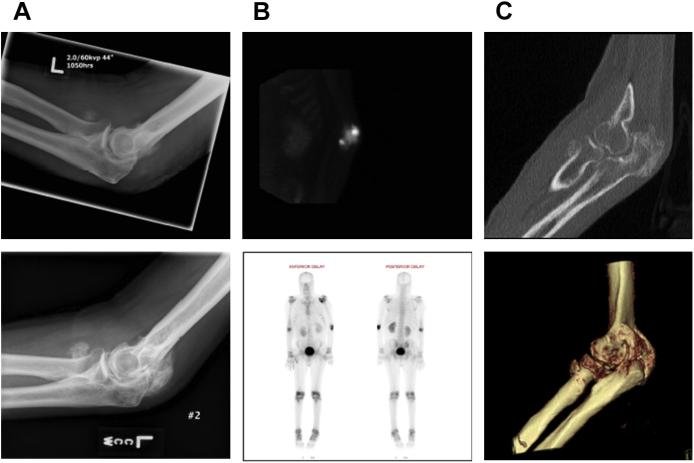
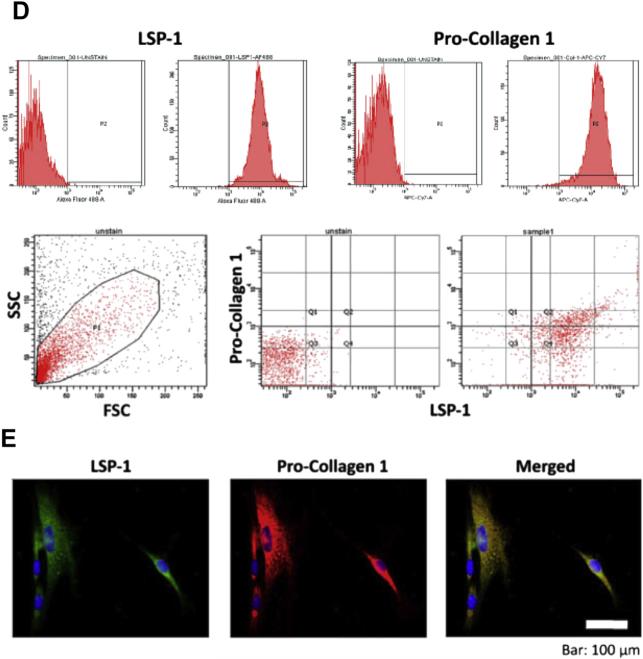
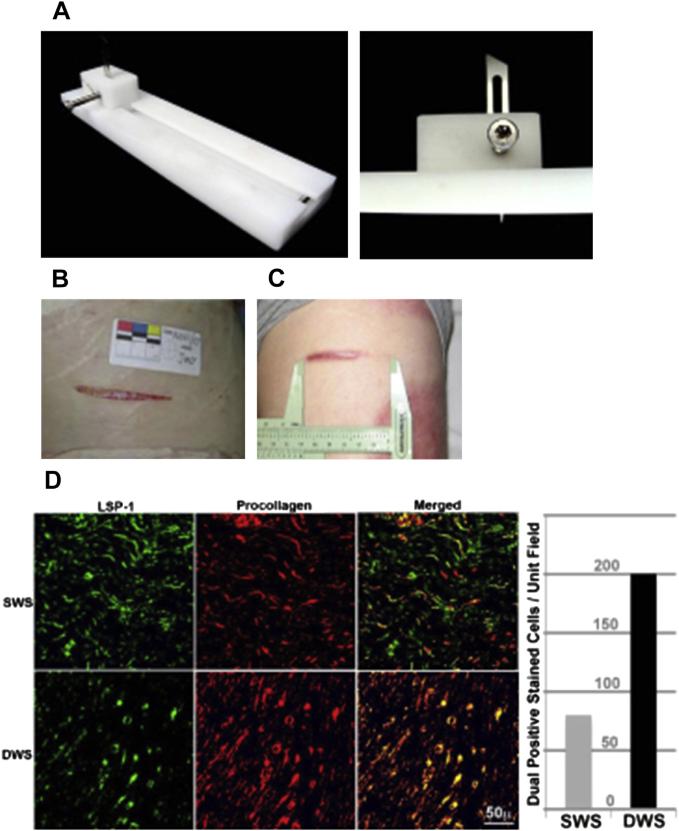
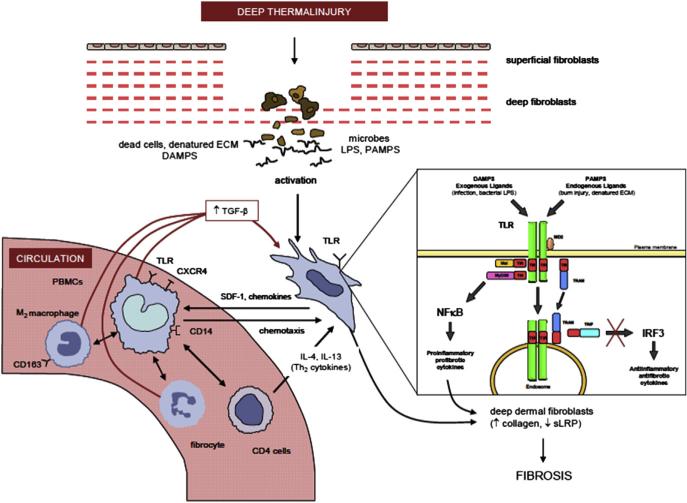
Hypertrophic scarring is extremely common and is the source of most morbidity related to burns. The biology of hypertrophic healing is complex and poorly understood. Multiple host and injury factors contribute, but protracted healing of partial thickness injury is a common theme. Hypertrophic scarring and heterotopic ossification may share some basic causes involving marrow-derived cells. Several traditional clinical interventions exist to modify hypertrophic scar. All have limited efficacy. Laser interventions for scar modification show promise, but as yet do not provide a definitive solution. Their efficacy is only seen when used as part of a multimodality scar management program.
Keywords: Burn reconstruction; Fibrocytes; Heterotopic ossification; Laser; Scar.
Crown Copyright © 2014. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kwan P, Desmouliere A, Tredget EE. Chapter 45—Molecular and cellular basis of hypertrophic scarring. In: Herndon DN, editor. Total burn care. 3rd edition. Saunders Elsevier; Philadelphia: 2012. pp. 495–505.e5.
-
- Bombaro KM, Engrav LH, Carrougher GJ, et al. What is the prevalence of hyper-trophic scarring following burns? Burns. 2003;29:299–302. - PubMed
-
- Engrav LH, Covey MH, Dutcher KD, et al. Impairment, time out of school, and time off from work after burns. Plast Reconstr Surg. 1987;79:927–34. - PubMed
-
- Helm P, Herndon DN, Delateur B. Restoration of function. J Burn Care Res. 2007;28(4):611–4. - PubMed
-
- Brown JJ, Bayat A. Genetic susceptibility to raised dermal scarring. Br J Dermatol. 2009;161(1):8–18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
