

Review
doi: 10.1101/cshperspect.a015354.
Psoriasis
Affiliations
- PMID: 25085957
- PMCID: PMC4109580
- DOI: 10.1101/cshperspect.a015354
Item in Clipboard
Review
Psoriasis
Cold Spring Harb Perspect Med.
.
Abstract
Psoriasis is a common chronic inflammatory skin disease with a spectrum of clinical phenotypes and results from the interplay of genetic, environmental, and immunological factors. Four decades of clinical and basic research on psoriasis have elucidated many of the pathogenic mechanisms underlying disease and paved the way to effective targeted therapies. Here, we review this progress and identify future directions of study that are supported by a more integrative research approach and aim at further improving the patients' life.
Copyright © 2014 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
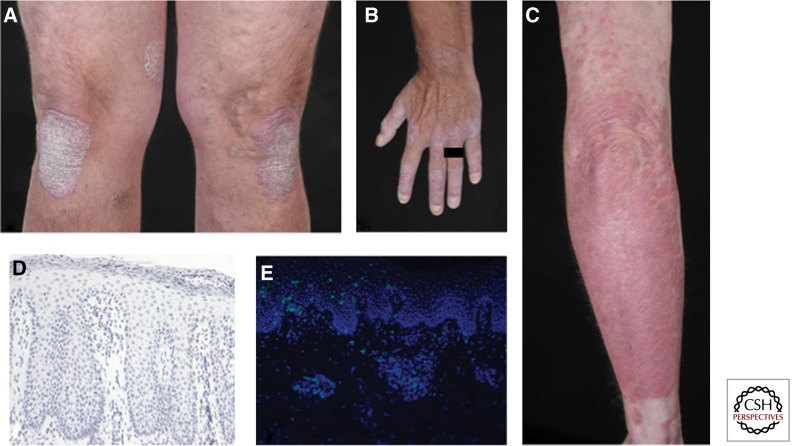
Clinical and histopathological features of psoriasis. (A–C) Clinical pictures of chronic plaque psoriasis. Note nail involvement in B. (D) Hematoxylin-stained section from a chronic psoriatic plaque. Typical histological features are visible: acanthosis, papillomatosis, parakeratosis, as well as Munro abscess in the stratum corneum. (E) Immunofluorescence staining of chronic psoriatic plaque showing skin infiltrating CD3+ T cells in green.
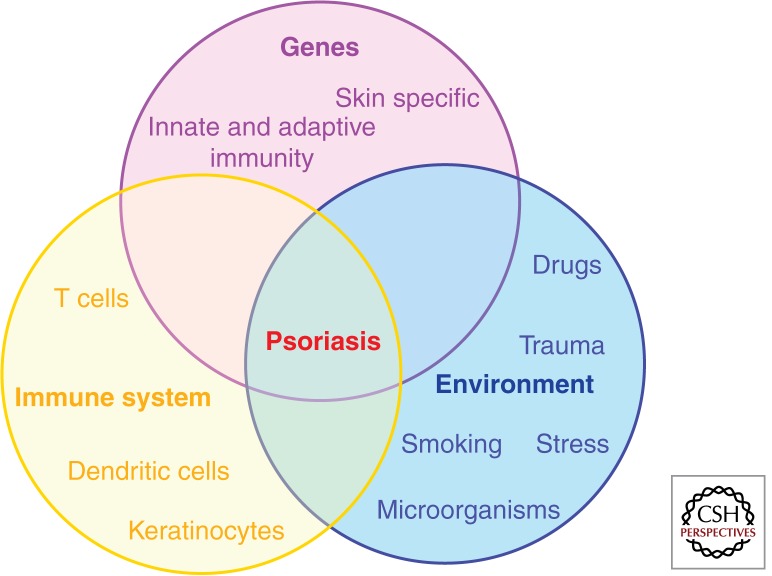
Psoriasis etiopathogenesis. Disease takes place in genetically predisposed individuals, carrying one or more psoriasis susceptibility genes (either skin specific or of immunological function) in which a dysregulated immune response (involving DC, T cells, and KCs) occurs, following exposure to certain environmental triggers.
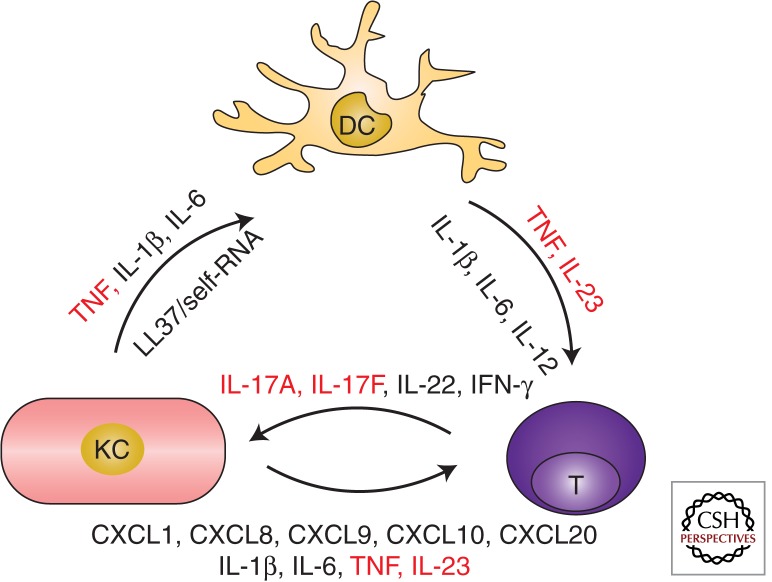
Psoriasis immunopathogenesis. A pathogenic cross talk between innate and adaptive immune cells, sustained by proinflammatory mediators, underlies the dysregulated immune response seen in psoriasis. The three main cellular players and their products are depicted in this diagram. KCs produce key cytokines (TNF, interleukin-[IL] 1β, and IL-6), as well as the AMP LL37-binding self-RNA activating myeloid DC in the dermis. Activated DC present, yet not identified, antigens and secrete mediators such as TNF, IL-23, IL-1β, IL-6 leading to the differentiation and activation of IL-17-producing T cells (T, here representing both αβ and γδ TCR T cells). T cells, in turn, secrete cytokines (IL-17A, IL-17F, IL-22, IFN-γ) that activate KC aberrant differentiation program and induce the production of further proinflammatory mediators, especially chemokines (CXCL1, CXCL8,) recruiting neutrophils (not shown) or other immune cells (CXCL9, CXCL10, CCL20), as well as other antimicrobial peptides (not shown). Critical proinflammatory molecules, effectively targeted by biologic drugs, are shown in red.
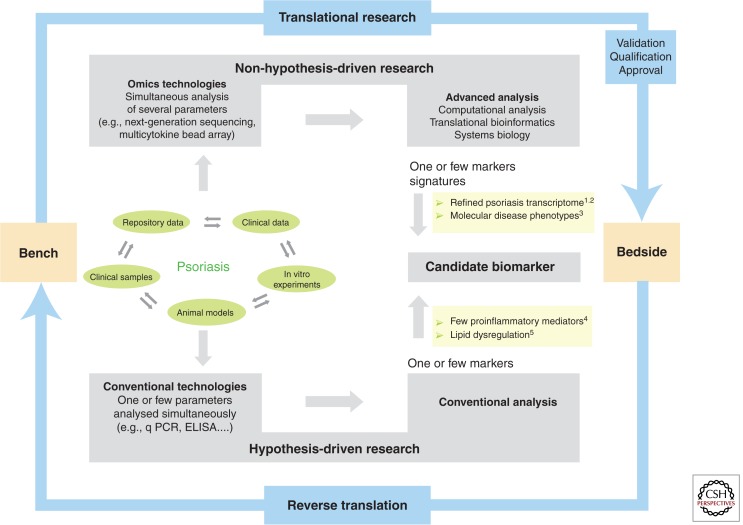
Psoriasis research for disease-specific biomarker discovery. Psoriasis research progresses via reciprocal inputs from the bench to the bedside (translational research) and vice versa (reverse translation). Clinical samples and data, repository data, in vitro, and in vivo animal models can be assessed and analyzed using conventional technologies measuring one or few parameters according to a preformed hypothesis, or innovative high-throughput platforms, which simultaneously measure many parameters according to a non–a priori hypothesis approach. Both strategies can lead to the identification of a candidate biomarker, which coincides with one, several, or multiple markers leading to molecular signatures in the case of omics data. Whatever the discovery approach, the clinical translation of a biomarker will then require the successful achievement of the validation, qualification, and approval process. Examples in the figure are from: 1Suarez-Farinas et al. 2012; 2Tian et al. 2012; 3Ainali et al. 2012; 4Arican et al. 2005; 5Gupta et al. 2011.
References
-
- Ahlehoff O, Gislason GH, Charlot M, Jorgensen CH, Lindhardsen J, Olesen JB, Abildstrom SZ, Skov L, Torp-Pedersen C, Hansen PR 2011. Psoriasis is associated with clinically significant cardiovascular risk: A Danish nationwide cohort study. J Intern Med 270: 147–157 - PubMed
-
- Amgen. 2013a. Study of efficacy and safety of brodalumab compared with placebo and ustekinumab in moderate to severe plaque psoriasis subjects (AMAGINE-2). clinicaltrials.gov/ct2/show/NCT01708603.
-
- Amgen. 2013b. Study of efficacy and safety of brodalumab compared with placebo and ustekinumab in moderate to severe plaque psoriasis subjects (AMAGINE-3). clinicaltrials.gov/ct2/show/NCT01708629.
-
- Amgen. 2013c. Study of efficacy, safety, and withdrawal and retreatment with brodalumab in moderate to severe plaque psoriasis subjects (AMAGINE-1). http://clinicaltrials.gov/ct2/show/NCT01708590.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases