

New concepts in the management of diffuse low-grade glioma: Proposal of a multistage and individualized therapeutic approach
- PMID: 25087230
- PMCID: PMC4483091
- DOI: 10.1093/neuonc/nou153
New concepts in the management of diffuse low-grade glioma: Proposal of a multistage and individualized therapeutic approach
Abstract
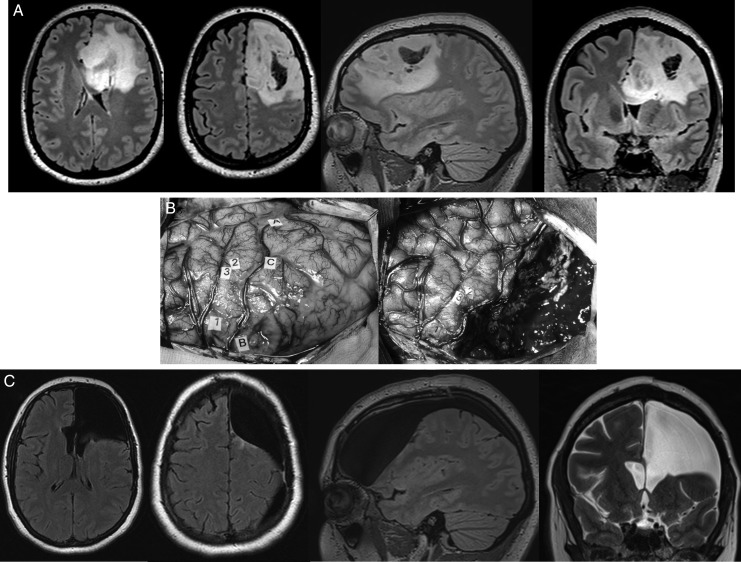
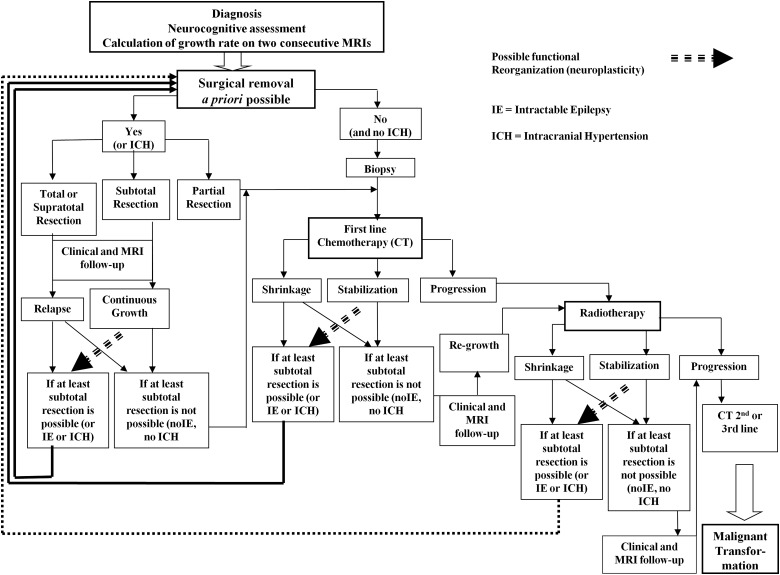
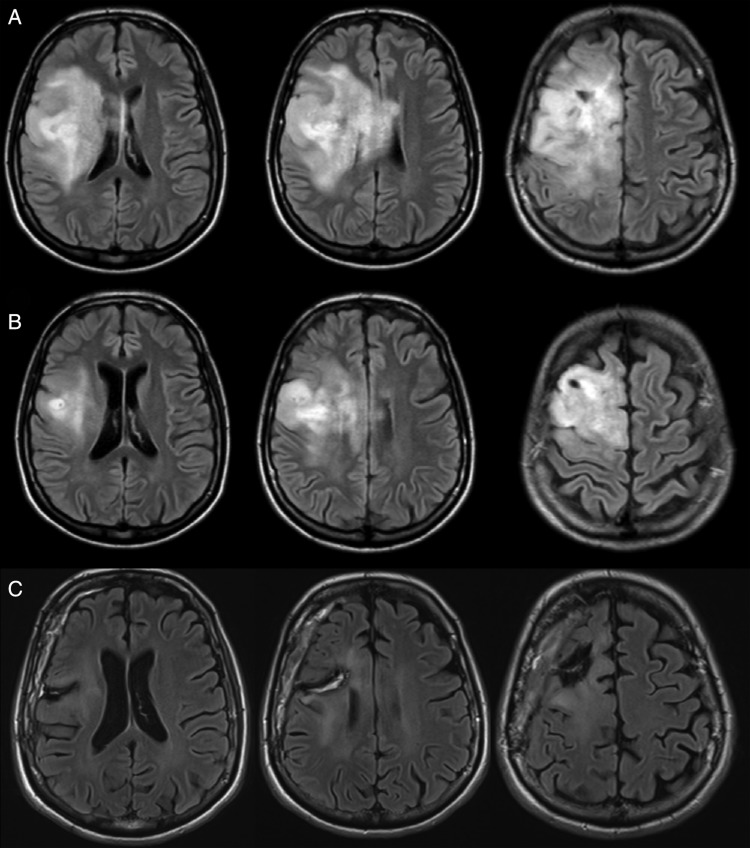
Diffuse low-grade glioma grows, migrates along white matter tracts, and progresses to high-grade glioma. Rather than a "wait and see" policy, an aggressive attitude is now recommended, with early surgery as the first therapy. Intraoperative mapping, with maximal resection according to functional boundaries, is associated with a longer overall survival (OS) while minimizing morbidity. However, most studies have investigated the role of only one specific treatment (surgery, radiotherapy, chemotherapy) without taking a global view of managing the cumulative time while preserving quality of life (QoL) versus time to anaplastic transformation. Our aim is to switch towards a more holistic concept based upon the anticipation of a personalized and long-term multistage therapeutic approach, with online adaptation of the strategy over the years using feedback from clinical, radiological, and histomolecular monitoring. This dynamic strategy challenges the traditional approach by proposing earlier therapy, by repeating treatments, and by reversing the classical order of therapies (eg, neoadjuvant chemotherapy when maximal resection is impossible, no early radiotherapy) to improve OS and QoL. New individualized management strategies should deal with the interactions between the course of this chronic disease, reaction brain remapping, and oncofunctional modulation elicited by serial treatments. This philosophy supports a personalized, functional, and preventive neuro-oncology.
Keywords: awake surgery; diffuse low-grade gliomas; individualized management; multistage therapeutic approach; quality of life.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Louis D, Ohgaki H, Wiestler O, et al. World Health Organization Classification of Tumors of the Central Nervous System. 4th ed. Lyon: IARC; 2007. - PubMed
-
- Duffau H. In: Diffuse Low Grade Glioma in Adults: Natural History, Interaction with the Brain, and New Individualized Therapeutic Strategies. Duffau H, editor. London: Springer; 2013.
-
- Rigau V. In: Histological Classification. In Diffuse Low Grade Glioma in Adults: Natural History, Interaction with the Brain, and New Individualized Therapeutic Strategies. Duffau H, editor. London: Springer; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
