

Renal endothelial dysfunction in acute kidney ischemia reperfusion injury
- PMID: 25088124
- PMCID: PMC4215733
- DOI: 10.2174/1871529x1401140724093505
Renal endothelial dysfunction in acute kidney ischemia reperfusion injury
Abstract
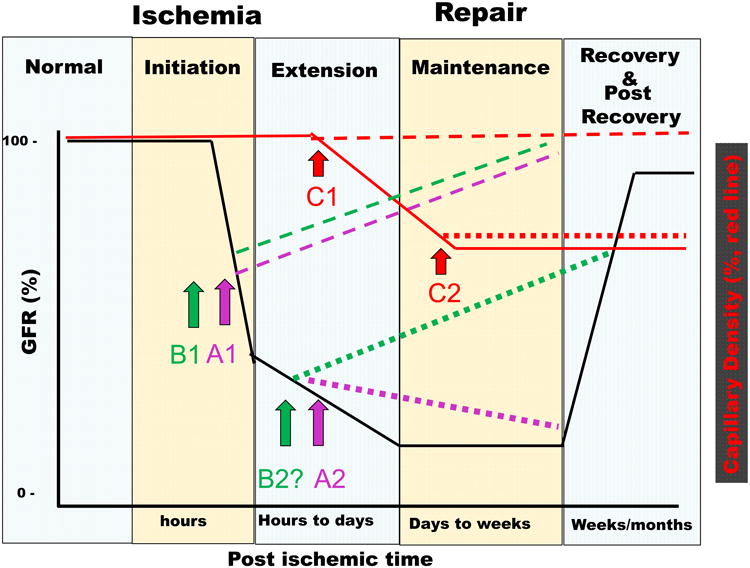
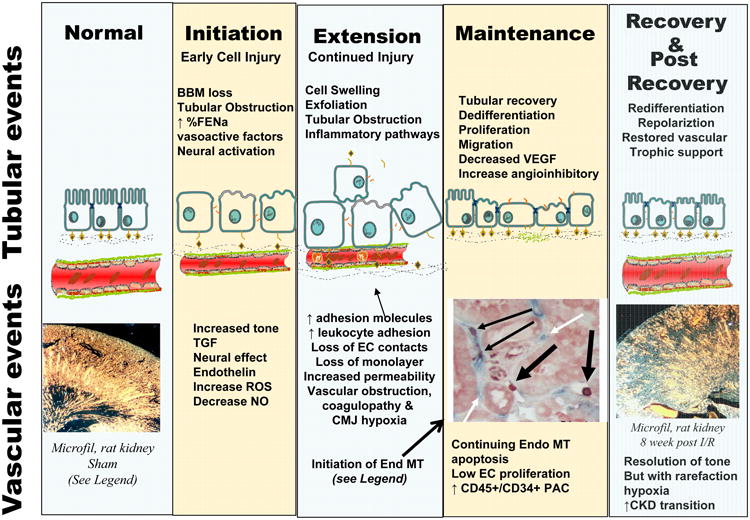
Acute kidney injury is associated with alterations in vascular tone that contribute to an overall reduction in GFR. Studies in animal models indicate that ischemia triggers alterations in endothelial function that contribute significantly to the overall degree and severity of a kidney injury. Putative mediators of vasoconstriction that may contribute to the initial loss of renal blood flow and GFR are highlighted. In addition, there is discussion of how intrinsic damage to the endothelium impairs homeostatic responses in vascular tone as well as promotes leukocyte adhesion and exacerbating the reduction in renal blood flow. The timing of potential therapies in animal models as they relate to the evolution of AKI, as well as the limitations of such approaches in the clinical setting are discussed. Finally, we discuss how acute kidney injury induces permanent alterations in renal vascular structure. We posit that the cause of the sustained impairment in kidney capillary density results from impaired endothelial growth responses and suggest that this limitation is a primary contributing feature underlying progression of chronic kidney disease.
Figures
References
-
- Liangos O, Wald R, O'Bell JW, Price L, Pereira BJ, Jaber BL. Epidemiology and Outcomes of Acute Renal Failure in Hospitalized Patients: A National Survey. Clinical Journal of the American Society of Nephrology. 2006;1(1):43–51. - PubMed
-
- Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA. 1996;275(19):1489–94. - PubMed
-
- Mehta RL, Chertow GM. Acute renal failure definitions and classification: time for change? J Am Soc Nephrol. 2003;14(8):2178–87. - PubMed
-
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
