

Multicenter development and validation of a risk stratification tool for ward patients
- PMID: 25089847
- PMCID: PMC4214112
- DOI: 10.1164/rccm.201406-1022OC
Multicenter development and validation of a risk stratification tool for ward patients
Abstract
Rationale: Most ward risk scores were created using subjective opinion in individual hospitals and only use vital signs.
Objectives: To develop and validate a risk score using commonly collected electronic health record data.
Methods: All patients hospitalized on the wards in five hospitals were included in this observational cohort study. Discrete-time survival analysis was used to predict the combined outcome of cardiac arrest (CA), intensive care unit (ICU) transfer, or death on the wards. Laboratory results, vital signs, and demographics were used as predictor variables. The model was developed in the first 60% of the data at each hospital and then validated in the remaining 40%. The final model was compared with the Modified Early Warning Score (MEWS) using the area under the receiver operating characteristic curve and the net reclassification index (NRI).
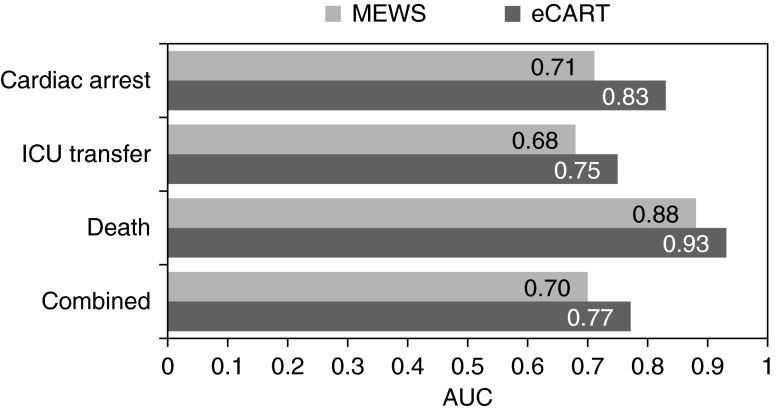
Measurements and main results: A total of 269,999 patient admissions were included, with 424 CAs, 13,188 ICU transfers, and 2,840 deaths occurring during the study period. The derived model was more accurate than the MEWS in the validation dataset for all outcomes (area under the receiver operating characteristic curve, 0.83 vs. 0.71 for CA; 0.75 vs. 0.68 for ICU transfer; 0.93 vs. 0.88 for death; and 0.77 vs. 0.70 for the combined outcome; P value < 0.01 for all comparisons). This accuracy improvement was seen across all hospitals. The NRI for the electronic Cardiac Arrest Risk Triage compared with the MEWS was 0.28 (0.18-0.38), with a positive NRI of 0.19 (0.09-0.29) and a negative NRI of 0.09 (0.09-0.09).
Conclusions: We developed an accurate ward risk stratification tool using commonly collected electronic health record variables in a large multicenter dataset. Further study is needed to determine whether implementation in real-time would improve patient outcomes.
Keywords: decision support techniques; early diagnosis; heart arrest; hospital rapid response team; statistical models.
Figures
Comment in
-
The art of making predictions: statistics versus bedside evaluation.Am J Respir Crit Care Med. 2014 Sep 15;190(6):598-9. doi: 10.1164/rccm.201408-1457ED. Am J Respir Crit Care Med. 2014. PMID: 25221875 No abstract available.
References
-
- Merchant RM, Yang L, Becker LB, Berg RA, Nadkarni V, Nichol G, Carr BG, Mitra N, Bradley SM, Abella BS, et al. American Heart Association Get With The Guidelines-Resuscitation Investigators. Incidence of treated cardiac arrest in hospitalized patients in the United States. Crit Care Med. 2011;39:2401–2406. - PMC - PubMed
-
- Berlot G, Pangher A, Petrucci L, Bussani R, Lucangelo U. Anticipating events of in-hospital cardiac arrest. Eur J Emerg Med. 2004;11:24–28. - PubMed
-
- Hodgetts TJ, Kenward G, Vlackonikolis I, Payne S, Castle N, Crouch R, Ineson N, Shaikh L. Incidence, location and reasons for avoidable in-hospital cardiac arrest in a district general hospital. Resuscitation. 2002;54:115–123. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
