

Cardiovascular risk factor burden in Africa and the Middle East: the Africa Middle East Cardiovascular Epidemiological (ACE) study
- PMID: 25090638
- PMCID: PMC4121128
- DOI: 10.1371/journal.pone.0102830
Cardiovascular risk factor burden in Africa and the Middle East: the Africa Middle East Cardiovascular Epidemiological (ACE) study
Abstract
Background: Increased urbanization in the developing world parallels a rising burden of chronic diseases. Developing countries account for ∼ 80% of global cardiovascular (CV) deaths, but contribute a paucity of systematic epidemiological data on CV risk factors.
Objective: To estimate the prevalence of CV risk factors in rural and urban cohorts attending general practice clinics in the Africa and Middle East (AfME) region.
Methods: In a cross-sectional epidemiological study, the presence of CV risk factors (hypertension, diabetes mellitus (diabetes), dyslipidemia, obesity, smoking and abdominal obesity) were evaluated in stable adult outpatients attending general practice primary care clinics. A rural population was defined as isolated (>50 km or lack of easy access to commuter transportation) from urban centers.
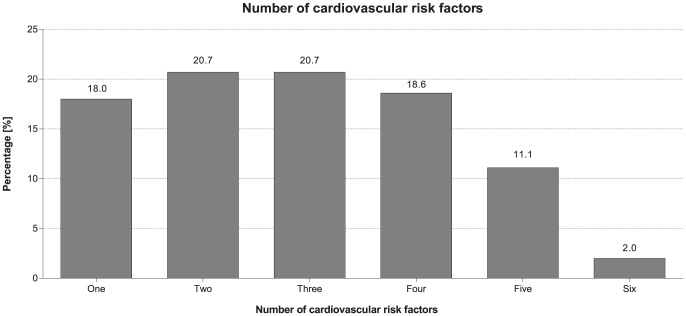
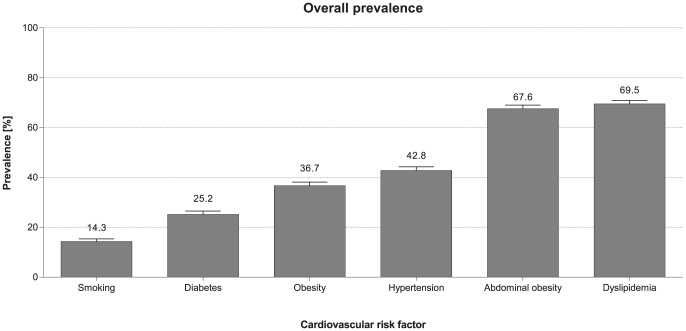
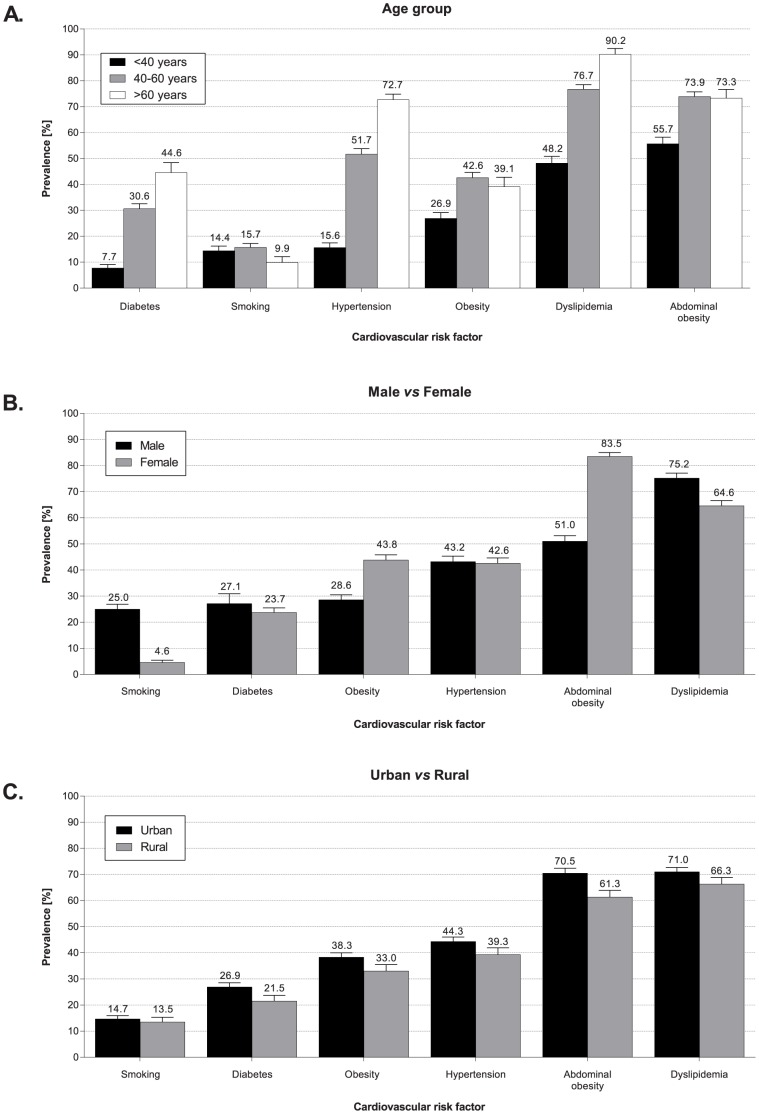
Results: 4,378 outpatients were systematically recruited from 94 clinics across 14 AfME countries. Mean age was 46 ± 14 years and 52% of outpatients were female. A high prevalence of dyslipidemia (70%) and abdominal obesity (68%) were observed, followed by hypertension (43%) and diabetes (25%). The vast majority of outpatients (92%) had at least one modifiable CV risk factor, many (74%) had more than one, and half (53%) had 3 or more. These findings were observed in both genders and across urban and rural centers. Among outpatients with pre-existing hypertension or dyslipidemia, many were not at their target blood pressure or LDL-cholesterol goals.
Conclusion: Cardiovascular risk factors are highly prevalent among relatively young, stable outpatients attending general practice clinics across AfME. The findings support opportunistic screening for CV risk factors whenever outpatients visit a general practitioner and provide an opportunity for early identification and management of CV risk factors, including lifestyle interventions.
Conflict of interest statement
Figures
References
-
- Levenson JW, Skerrett PJ, Gaziano M (2002) Reducing the Global Burden of Cardiovascular Disease: The Role of Risk Factors. Prev Cardiol 5: 188–99. - PubMed
-
- Yusuf S, Reddy S, Ounpuu S, Anand S (2001) Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 104: 2746–53. - PubMed
-
- Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K (2007) The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370: 1929–38. - PubMed
-
- Gaziano TA (2005) Cardiovascular disease in the developing world and its cost-effective management. Circulation 112: 3547–53. - PubMed
-
- World Health Organization (2006) Country Cooperation Strategy for WHO and Saudi Arabia 2006–2011. Available: http://www.who.int/countryfocus/cooperation_strategy/ccs_sau_en.pdf. Accessed 19 November 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
