

Banff Initiative for Quality Assurance in Transplantation (BIFQUIT): reproducibility of polyomavirus immunohistochemistry in kidney allografts
- PMID: 25091177
- PMCID: PMC4194133
- DOI: 10.1111/ajt.12794
Banff Initiative for Quality Assurance in Transplantation (BIFQUIT): reproducibility of polyomavirus immunohistochemistry in kidney allografts
Abstract
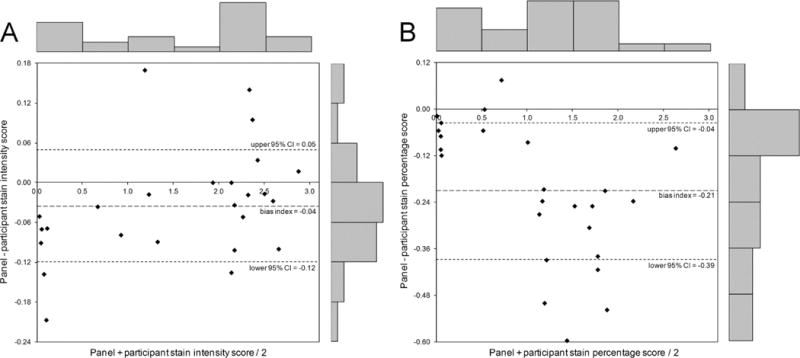
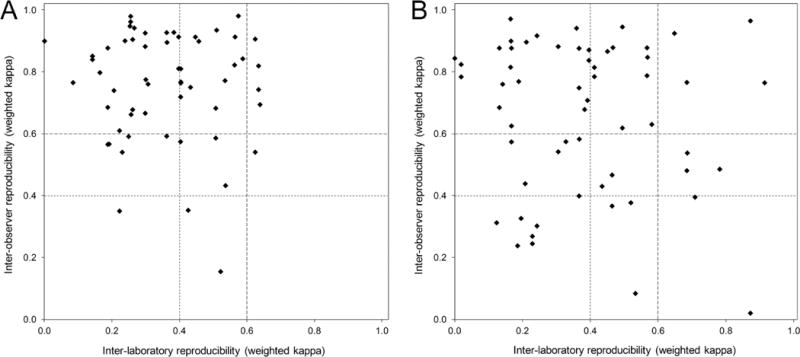
Immunohistochemistry (IHC) is the gold standard for diagnosing (positive vs. negative) polyomavirus BK (BKV) nephropathy and has the potential for disease staging based on staining intensity and quantification of infected cells. This multicenter trial evaluated the reproducibility of BKV IHC among 81 pathologists at 60 institutions. Participants stained tissue microarray slides and scored them for staining intensity and percentage of positive nuclei. Staining protocol details and evaluation scores were collected online. Slides were returned for centralized panel re-evaluation and kappa statistics were calculated. Individual assessment of staining intensity and percentage was more reproducible than combined scoring. Inter-institutional reproducibility was moderate for staining intensity (κ = 0.49) and percentage (κ = 0.42), fair for combined (κ = 0.25) and best for simple positive/negative scoring (κ = 0.78). Inter-observer reproducibility was substantial for intensity (κ = 0.74), percentage (κ = 0.66), positive/negative (κ = 0.78) and moderate for combined scoring (κ = 0.43). Inter-laboratory reproducibility was fair for intensity (κ = 0.37), percentage (κ = 0.40) and combined (κ = 0.24), but substantial for positive/negative scoring (κ = 0.67). BKV RNA copies/cell correlated with staining intensity (r = 0.56) and percentage (r = 0.62). These results indicate that BKV IHC is reproducible between observers but scoring should be simplified to a single-feature schema. Standardization of tissue processing and staining protocols would further improve inter-laboratory reproducibility.
Keywords: Clinical research/practice; infection and infectious agents; kidney (allograft) function/dysfunction; kidney disease: infectious; pathology/histopathology; viral: BK/JC/polyoma.
© Copyright 2014 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have conflicts of interest to disclose as described by the
Figures

References
-
- Brennan DC, Agha I, Bohl DL, Schnitzler MA, Hardinger KL, Lockwood M, et al. Incidence of BK with tacrolimus versus cyclosporine and impact of preemptive immunosuppression reduction. Am J Transplant. 2005;5(3):582–94. - PubMed
-
- Drachenberg CB, Papadimitriou JC, Hirsch HH, Wali R, Crowder C, Nogueira J, et al. Histological patterns of polyomavirus nephropathy: correlation with graft outcome and viral load. Am J Transplant. 2004;4(12):2082–92. - PubMed
-
- Hariharan S. BK virus nephritis after renal transplantation. Kidney Int. 2006;69(4):655–62. - PubMed
-
- Buehrig CK, Lager DJ, Stegall MD, Kreps MA, Kremers WK, Gloor JM, et al. Influence of surveillance renal allograft biopsy on diagnosis and prognosis of polyomavirus-associated nephropathy. Kidney Int. 2003;64(2):665–73. - PubMed
-
- Hirsch HH, Randhawa P. BK virus in solid organ transplant recipients. Am J Transplant. 2009;9(Suppl 4):S136–S146. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
