

Surgery for hip fracture yields societal benefits that exceed the direct medical costs
- PMID: 25091223
- PMCID: PMC4182375
- DOI: 10.1007/s11999-014-3820-6
Surgery for hip fracture yields societal benefits that exceed the direct medical costs
Abstract
Background: A hip fracture is a debilitating condition that consumes significant resources in the United States. Surgical treatment of hip fractures can achieve better survival and functional outcomes than nonoperative treatment, but less is known about its economic benefits.
Questions/purposes: We asked: (1) Are the societal benefits of hip fracture surgery enough to offset the direct medical costs? (2) Nationally, what are the total lifetime benefits of hip fracture surgery for a cohort of patients and to whom do these benefits accrue?
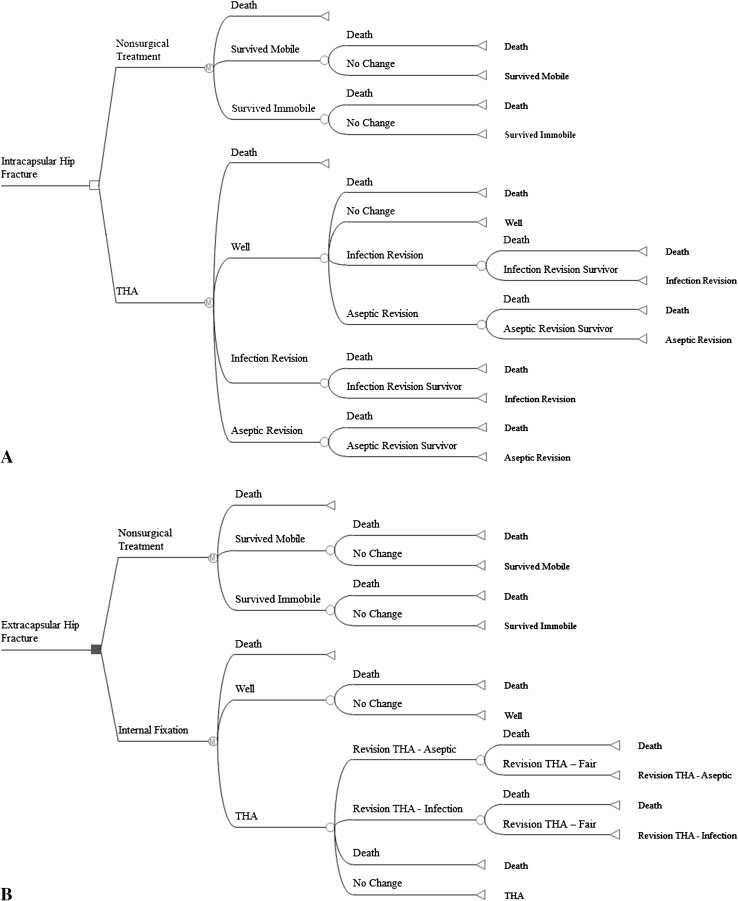
Methods: We estimated the effects of surgical treatment for displaced hip fractures through a Markov cohort analysis of patients 65 years and older. Assumptions were obtained from a systematic literature review, analysis of Medicare claims data, and clinical experts. We conducted a series sensitivity analyses to assess the effect of uncertainty in model parameters on our estimates. We compared costs for medical care, home modification, and long-term nursing home use for surgical and nonoperative treatment of hip fractures to estimate total societal savings.
Results: Estimated average lifetime societal benefits per patient exceeded the direct medical costs of hip fracture surgery by USD 65,000 to USD 68,000 for displaced hip fractures. With the exception of the assumption of nursing home use, the sensitivity analyses show that surgery produces positive net societal savings with significant deviations of 50% from the base model assumptions. For an 80-year-old patient, the breakeven point for the assumption on the percent of patients with hip fractures who would require long-term nursing home use with nonoperative treatment is 37% to 39%, compared with 24% for surgical patients. Nationally, we estimate that hip fracture surgery for the cohort of patients in 2009 yields lifetime societal savings of USD 16 billion in our base model, with benefits and direct costs of USD 21 billion and USD 5 billion, respectively. For an 80-year-old, societal benefits ranged from USD 2 billion to USD 32 billion, using our range of estimates for nursing home use among nonoperatively treated patients who are immobile after the fracture.
Conclusions: Surgical treatment of hip fractures produces societal savings. Although the magnitude of these savings depends on model assumptions, the finding of societal savings is robust to a range of parameter values.
Level of evidence: Level III, economic and decision analyses. See the Instructions for Authors for a complete description of levels of evidence.
Figures
Comment in
-
CORR Insights®: surgery for hip fracture yields societal benefits that exceed the direct medical costs.Clin Orthop Relat Res. 2014 Nov;472(11):3547-8. doi: 10.1007/s11999-014-3896-z. Epub 2014 Sep 3. Clin Orthop Relat Res. 2014. PMID: 25183218 Free PMC article. No abstract available.
References
-
- Agency for Healthcare Research and Quality. Calculating the U.S. population-based EQ-5D™ index score. Available at: http://www.ahrq.gov/rice/EQ5Dscore.htm. Accessed April 23, 2012.
-
- Agency for Healthcare Research and Quality. National and regional estimates on hospital use for all patients from the HCUP Nationwide Inpatient Sample (NIS). Available at: http://hcupnet.ahrq.gov/HCUPnet.jsp. Accessed July 26, 2012.
-
- Arias E. United States life tables, 2007. Natl Vital Stat Rep. 2011;59:1–60. - PubMed
-
- Bentler S, Liu L, Obrizan M, Cook EA, Wright KB, Geweke JF, Chrischilles EA, Pavlik CE, Wallace RB, Ohsfeldt RL, Jones MP, Rosenthal GE, Wolinsky FD. The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am J Epidemiol. 2009;170:1290–1299. doi: 10.1093/aje/kwp266. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
