

Systemic therapy of Cushing's syndrome
- PMID: 25091295
- PMCID: PMC4237936
- DOI: 10.1186/s13023-014-0122-8
Systemic therapy of Cushing's syndrome
Abstract
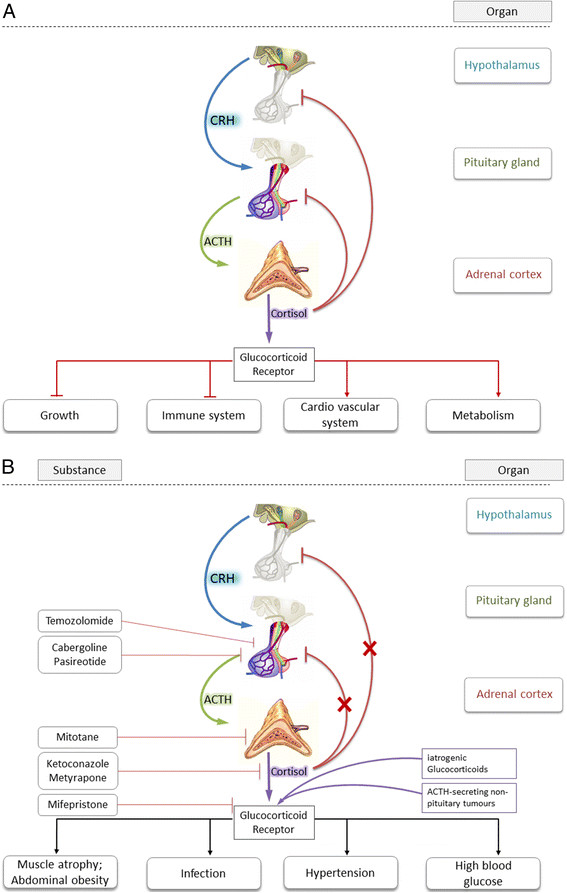
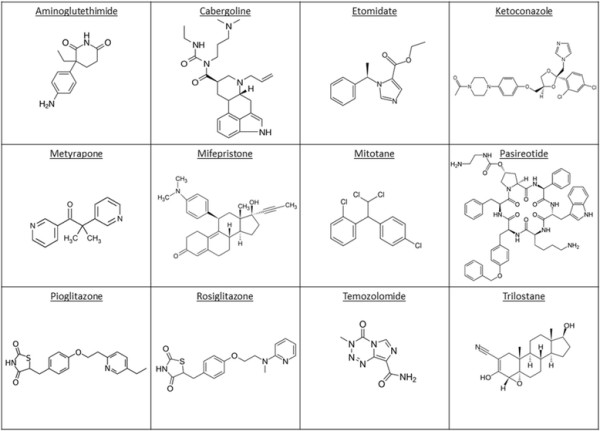
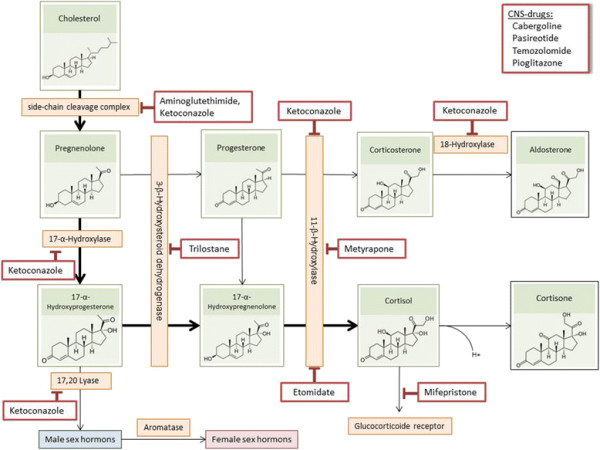
Cushing's disease (CD) in a stricter sense derives from pathologic adrenocorticotropic hormone (ACTH) secretion usually triggered by micro- or macroadenoma of the pituitary gland. It is, thus, a form of secondary hypercortisolism. In contrast, Cushing's syndrome (CS) describes the complexity of clinical consequences triggered by excessive cortisol blood levels over extended periods of time irrespective of their origin. CS is a rare disease according to the European orphan regulation affecting not more than 5/10,000 persons in Europe. CD most commonly affects adults aged 20-50 years with a marked female preponderance (1:5 ratio of male vs. female). Patient presentation and clinical symptoms substantially vary depending on duration and plasma levels of cortisol. In 80% of cases CS is ACTH-dependent and in 20% of cases it is ACTH-independent, respectively. Endogenous CS usually is a result of a pituitary tumor. Clinical manifestation of CS, apart from corticotropin-releasing hormone (CRH-), ACTH-, and cortisol-producing (malign and benign) tumors may also be by exogenous glucocorticoid intake. Diagnosis of hypercortisolism (irrespective of its origin) comprises the following: Complete blood count including serum electrolytes, blood sugar etc., urinary free cortisol (UFC) from 24 h-urine sampling and circadian profile of plasma cortisol, plasma ACTH, dehydroepiandrosterone, testosterone itself, and urine steroid profile, Low-Dose-Dexamethasone-Test, High-Dose-Dexamethasone-Test, after endocrine diagnostic tests: magnetic resonance imaging (MRI), ultra-sound, computer tomography (CT) and other localization diagnostics. First-line therapy is trans-sphenoidal surgery (TSS) of the pituitary adenoma (in case of ACTH-producing tumors). In patients not amenable for surgery radiotherapy remains an option. Pharmacological therapy applies when these two options are not amenable or refused. In cases when pharmacological therapy becomes necessary, Pasireotide should be used in first-line in CD. CS patients are at an overall 4-fold higher mortality rate than age- and gender-matched subjects in the general population. The following article describes the most prominent substances used for clinical management of CS and gives a systematic overview of safety profiles, pharmacokinetic (PK)-parameters, and regulatory framework.
Figures
Similar articles
-
Classic and recent etiologies of Cushing's syndrome: diagnosis and therapy.Treat Endocrinol. 2002;1(2):79-94. doi: 10.2165/00024677-200201020-00002. Treat Endocrinol. 2002. PMID: 15765624 Review.
-
Diagnosis and management of Cushing's syndrome: results of an Italian multicentre study. Study Group of the Italian Society of Endocrinology on the Pathophysiology of the Hypothalamic-Pituitary-Adrenal Axis.J Clin Endocrinol Metab. 1999 Feb;84(2):440-8. doi: 10.1210/jcem.84.2.5465. J Clin Endocrinol Metab. 1999. PMID: 10022398
-
[The ectopic ACTH syndrome].Srp Arh Celok Lek. 2004 Jan-Feb;132(1-2):28-32. doi: 10.2298/sarh0402028p. Srp Arh Celok Lek. 2004. PMID: 15227962 Serbian.
-
A very high dose dexamethasone suppression test for differential diagnosis of Cushing's syndrome.Clin Endocrinol (Oxf). 1998 Jan;48(1):45-51. doi: 10.1046/j.1365-2265.1998.00345.x. Clin Endocrinol (Oxf). 1998. PMID: 9509067
-
[Cushing's syndrome: diagnostic exploration].Presse Med. 1994 Jan 8-15;23(1):43-8. Presse Med. 1994. PMID: 8127815 Review. French.
Cited by
-
Cortisol as a Target for Treating Mental Disorders: A Promising Avenue for Therapy.Mini Rev Med Chem. 2024;24(6):588-600. doi: 10.2174/0113895575262104230928042150. Mini Rev Med Chem. 2024. PMID: 37861053 Review.
-
Whole organism transcriptome analysis of zebrafish models of Bardet-Biedl Syndrome and Alström Syndrome provides mechanistic insight into shared and divergent phenotypes.BMC Genomics. 2016 May 3;17:318. doi: 10.1186/s12864-016-2679-1. BMC Genomics. 2016. PMID: 27142762 Free PMC article.
-
Analysis of therapeutic effectiveness and adverse effects of long-term corticosteroids among leprosy patients with reactions: A retrospective cohort study.SAGE Open Med. 2022 Apr 19;10:20503121221089448. doi: 10.1177/20503121221089448. eCollection 2022. SAGE Open Med. 2022. PMID: 35465634 Free PMC article.
-
Deletion of the serine protease CAP2/Tmprss4 leads to dysregulated renal water handling upon dietary potassium depletion.Sci Rep. 2019 Dec 20;9(1):19540. doi: 10.1038/s41598-019-55995-x. Sci Rep. 2019. PMID: 31863073 Free PMC article.
-
Sexual dysfunction and male infertility.Nat Rev Urol. 2018 May;15(5):287-307. doi: 10.1038/nrurol.2018.20. Epub 2018 Mar 13. Nat Rev Urol. 2018. PMID: 29532805 Review.
References
-
- Purnell JQ, Brandon DD, Isabelle LM, Loriaux DL, Samuels MH. Association of 24-hour cortisol production rates, cortisol-binding globulin, and plasma-free cortisol levels with body composition, leptin levels, and aging in adult men and women. J Clin Endocrinol Metab. 2004;89:281–287. doi: 10.1210/jc.2003-030440. - DOI - PubMed
-
- Jackman S, Diamond F. Pituitary adenomas in childhood and adolescence. Pediatr Endocrinol Rev. 2013;10:450–459. - PubMed
-
- Mazziotti G, Giustina A. Glucocorticoids and the regulation of growth hormone secretion. Nat Rev Endocrinol. 2013;9:265–276. - PubMed
-
- Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319–327. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
