

Acute muscular sarcocystosis: an international investigation among ill travelers returning from Tioman Island, Malaysia, 2011-2012
- PMID: 25091309
- PMCID: PMC4624310
- DOI: 10.1093/cid/ciu622
Acute muscular sarcocystosis: an international investigation among ill travelers returning from Tioman Island, Malaysia, 2011-2012
Abstract
Background: Through 2 international traveler-focused surveillance networks (GeoSentinel and TropNet), we identified and investigated a large outbreak of acute muscular sarcocystosis (AMS), a rarely reported zoonosis caused by a protozoan parasite of the genus Sarcocystis, associated with travel to Tioman Island, Malaysia, during 2011-2012.
Methods: Clinicians reporting patients with suspected AMS to GeoSentinel submitted demographic, clinical, itinerary, and exposure data. We defined a probable case as travel to Tioman Island after 1 March 2011, eosinophilia (>5%), clinical or laboratory-supported myositis, and negative trichinellosis serology. Case confirmation required histologic observation of sarcocysts or isolation of Sarcocystis species DNA from muscle biopsy.
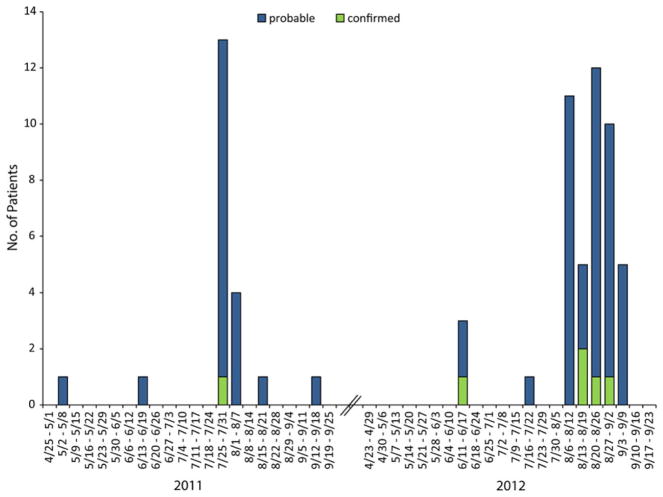
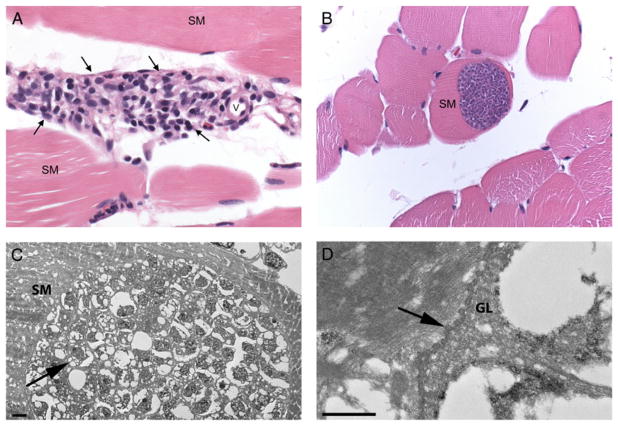
Results: Sixty-eight patients met the case definition (62 probable and 6 confirmed). All but 2 resided in Europe; all were tourists and traveled mostly during the summer months. The most frequent symptoms reported were myalgia (100%), fatigue (91%), fever (82%), headache (59%), and arthralgia (29%); onset clustered during 2 distinct periods: "early" during the second and "late" during the sixth week after departure from the island. Blood eosinophilia and elevated serum creatinine phosphokinase (CPK) levels were observed beginning during the fifth week after departure. Sarcocystis nesbitti DNA was recovered from 1 muscle biopsy.
Conclusions: Clinicians evaluating travelers returning ill from Malaysia with myalgia, with or without fever, should consider AMS, noting the apparent biphasic aspect of the disease, the later onset of elevated CPK and eosinophilia, and the possibility for relapses. The exact source of infection among travelers to Tioman Island remains unclear but needs to be determined to prevent future illnesses.
Keywords: Malaysia; infectious disease outbreak; parasitic disease; sarcocystosis; travel.
Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2014. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Conflict of interest statement
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures



Comment in
-
Prolonged clinical course of muscular sarcocystosis and effectiveness of cotrimoxazole among travelers to Tioman Island, Malaysia, 2011-2014.Clin Infect Dis. 2015 Jan 15;60(2):329. doi: 10.1093/cid/ciu791. Epub 2014 Oct 9. Clin Infect Dis. 2015. PMID: 25301217 Free PMC article. No abstract available.
-
Avoid haste in defining human muscular sarcocystosis.Clin Infect Dis. 2015 Apr 1;60(7):1134. doi: 10.1093/cid/ciu1163. Epub 2014 Dec 23. Clin Infect Dis. 2015. PMID: 25537869 No abstract available.
-
Reply to Italiano et al.Clin Infect Dis. 2015 Apr 1;60(7):1135-6. doi: 10.1093/cid/ciu1165. Epub 2014 Dec 23. Clin Infect Dis. 2015. PMID: 25537874 Free PMC article. No abstract available.
References
-
- Harvey K, Esposito DH, Han PV, et al. United States 1997–2011. MMWR Morb Mortal Wkly Rep. 2013;62:1–23. - PubMed
-
- Centers for Disease Control and Prevention. Notes from the field: acute muscular sarcocystosis among returning travelers—Tioman Island, Malaysia, 2011. MMWR Morb Mortal Wkly Rep. 2012;61:37. - PubMed
-
- Dubey JP, Speer CA, Fayer R. Sarcocystosis of animals and man. Boca Raton, FL: CRC Press, Inc; 1989.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
