

Coronary artery disease and diabetes mellitus
- PMID: 25091969
- PMCID: PMC4672945
- DOI: 10.1016/j.ccl.2014.04.001
Coronary artery disease and diabetes mellitus
Abstract
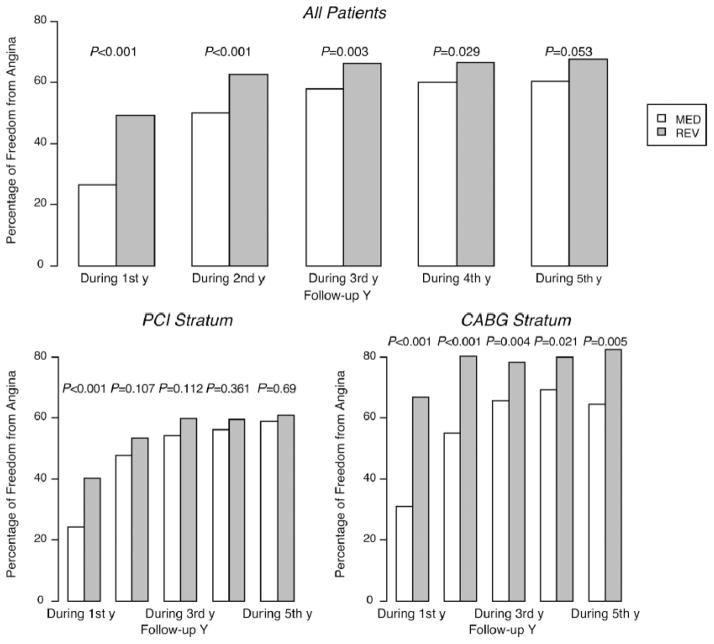
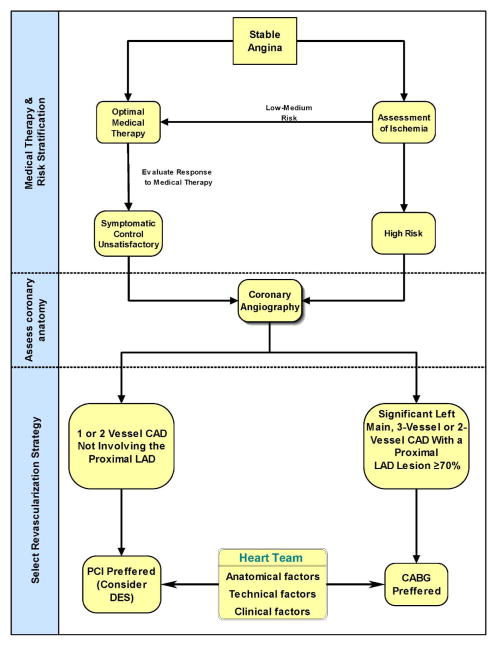
Diabetes mellitus (DM) is a major risk factor for cardiovascular disease. Near-normal glycemic control does not reduce cardiovascular events. For many patients with 1- or 2-vessel coronary artery disease, there is little benefit from any revascularization procedure over optimal medical therapy. For multivessel coronary disease, randomized trials demonstrated the superiority of coronary artery bypass grafting over multivessel percutaneous coronary intervention in patients with treated DM. However, selection of the optimal myocardial revascularization strategy requires a multidisciplinary team approach ('heart team'). This review summarizes the current evidence regarding the effectiveness of various medical therapies and revascularization strategies in patients with DM.
Keywords: Blood glucose; Coronary disease; Diabetes mellitus; Hypoglycemic agents; Revascularization; Statins.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
Republished in
-
Coronary Artery Disease and Diabetes Mellitus.Heart Fail Clin. 2016 Jan;12(1):117-33. doi: 10.1016/j.hfc.2015.08.010. Heart Fail Clin. 2016. PMID: 26567979 Review.
References
-
- Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40. - PubMed
-
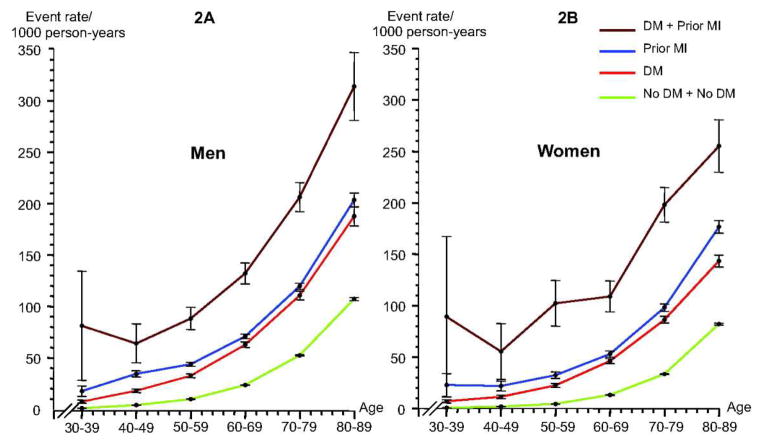
- Schramm TK, Gislason GH, Kober L, et al. Diabetes patients requiring glucose-lowering therapy and nondiabetics with a prior myocardial infarction carry the same cardiovascular risk: a population study of 3.3 million people. Circulation. 2008;117:1945–1954. - PubMed
-
- Berry C, Tardif JC, Bourassa MG. Coronary heart disease in patients with diabetes: part II: recent advances in coronary revascularization. J Am Coll Cardiol. 2007;49:643–656. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
