

Disparities in stage at diagnosis, treatment, and survival in nonelderly adult patients with cancer according to insurance status
- PMID: 25092774
- PMCID: PMC4876335
- DOI: 10.1200/JCO.2014.55.6258
Disparities in stage at diagnosis, treatment, and survival in nonelderly adult patients with cancer according to insurance status
Abstract
Purpose: The purpose of this study was to determine the association of insurance status with disease stage at presentation, treatment, and survival among the top 10 most deadly cancers using the SEER database.
Patients and methods: A total of 473,722 patients age 18 to 64 years who were diagnosed with one of the 10 most deadly cancers in the SEER database from 2007 to 2010 were analyzed. A Cox proportional hazards model was used for multivariable analyses to assess the effect of patient and tumor characteristics on cause-specific death.
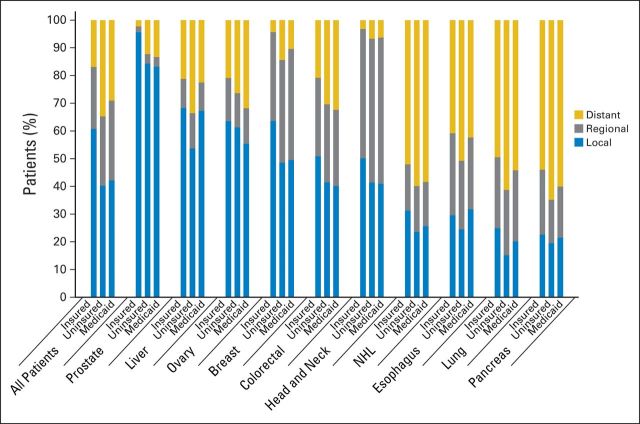
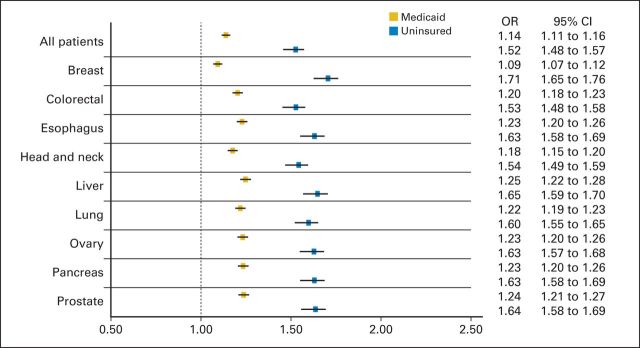
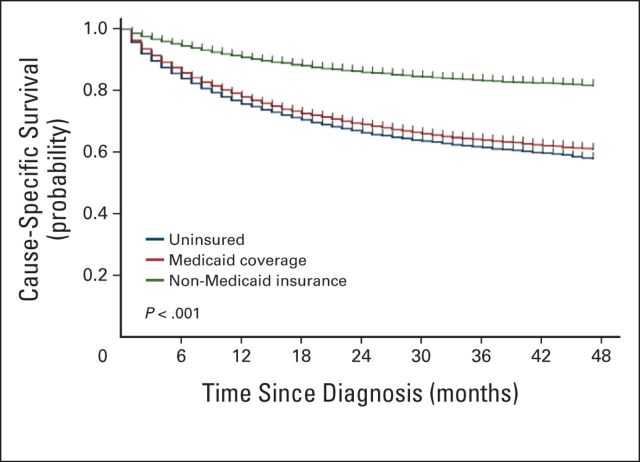
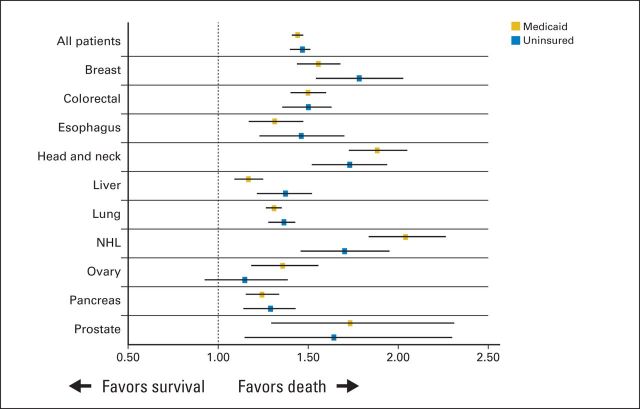
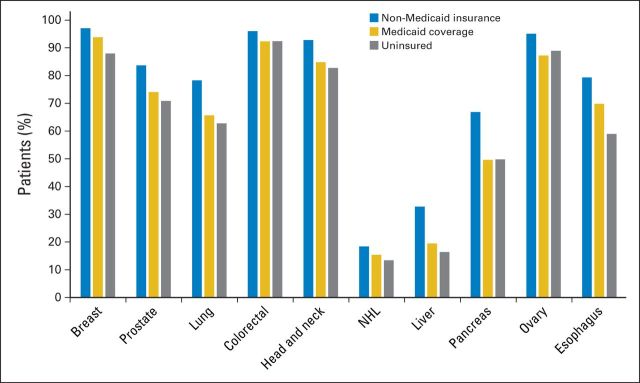
Results: Overall, patients with non-Medicaid insurance were less likely to present with distant disease (16.9%) than those with Medicaid coverage (29.1%) or without insurance coverage (34.7%; P < .001). Patients with non-Medicaid insurance were more likely to receive cancer-directed surgery and/or radiation therapy (79.6%) compared with those with Medicaid coverage (67.9%) or without insurance coverage (62.1%; P < .001). In a Cox regression that adjusted for age, race, sex, marital status, residence, percent of county below federal poverty level, site, stage, and receipt of cancer-directed surgery and/or radiation therapy, patients were more likely to die as a result of their disease if they had Medicaid coverage (hazard ratio [HR], 1.44; 95% CI, 1.41 to 1.47; P < .001) or no insurance (HR, 1.47; 95% CI, 1.42 to 1.51; P < .001) compared with non-Medicaid insurance.
Conclusion: Among patients with the 10 most deadly cancers, those with Medicaid coverage or without insurance were more likely to present with advanced disease, were less likely to receive cancer-directed surgery and/or radiation therapy, and experienced worse survival.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Inferior cancer outcomes more common for uninsured and Medicaid patients.CA Cancer J Clin. 2015 May-Jun;65(3):165-6. doi: 10.3322/caac.21270. Epub 2015 Mar 3. CA Cancer J Clin. 2015. PMID: 25737340 No abstract available.
-
Re: Disparities in Stage at Diagnosis, Treatment, and Survival in Nonelderly Adult Patients with Cancer According to Insurance Status.J Urol. 2015 Aug;194(2):501-2. doi: 10.1016/j.juro.2015.04.053. Epub 2015 Apr 15. J Urol. 2015. PMID: 26195419 No abstract available.
References
-
- DeNavas-Walt C, Proctor BD, Smith JC. Income, Poverty, and Health Insurance Coverage in the United States: 2012. http://www.census.gov/prod/2013pubs/p60-245.pdf.
-
- Patient Protection and Affordable Care Act. Pub Law 111-148.
-
- Hoyert DL, Xu J. Deaths: Preliminary Data for 2011. http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_06.pdf. - PubMed
-
- Ward EM, Fedewa SA, Cokkinides V, et al. The association of insurance and stage at diagnosis among patients aged 55 to 74 years in the national cancer database. Cancer J. 2010;16:614–621. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
