

Epidemiology, genetics, and subtyping of preserved ratio impaired spirometry (PRISm) in COPDGene
- PMID: 25096860
- PMCID: PMC4256936
- DOI: 10.1186/s12931-014-0089-y
Epidemiology, genetics, and subtyping of preserved ratio impaired spirometry (PRISm) in COPDGene
Abstract
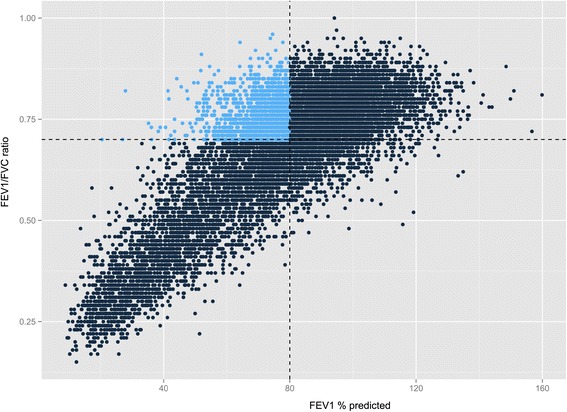
Background: Preserved Ratio Impaired Spirometry (PRISm), defined as a reduced FEV1 in the setting of a preserved FEV1/FVC ratio, is highly prevalent and is associated with increased respiratory symptoms, systemic inflammation, and mortality. Studies investigating quantitative chest tomographic features, genetic associations, and subtypes in PRISm subjects have not been reported.
Methods: Data from current and former smokers enrolled in COPDGene (n = 10,192), an observational, cross-sectional study which recruited subjects aged 45-80 with ≥10 pack years of smoking, were analyzed. To identify epidemiological and radiographic predictors of PRISm, we performed univariate and multivariate analyses comparing PRISm subjects both to control subjects with normal spirometry and to subjects with COPD. To investigate common genetic predictors of PRISm, we performed a genome-wide association study (GWAS). To explore potential subgroups within PRISm, we performed unsupervised k-means clustering.
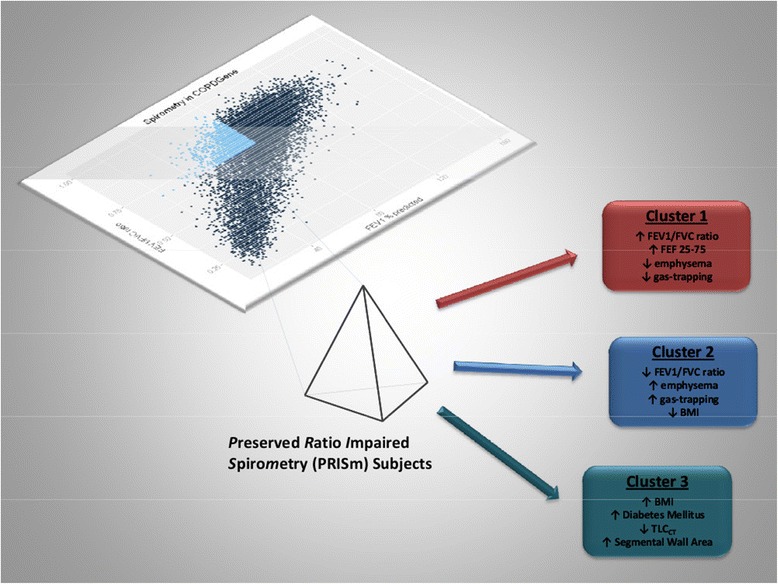
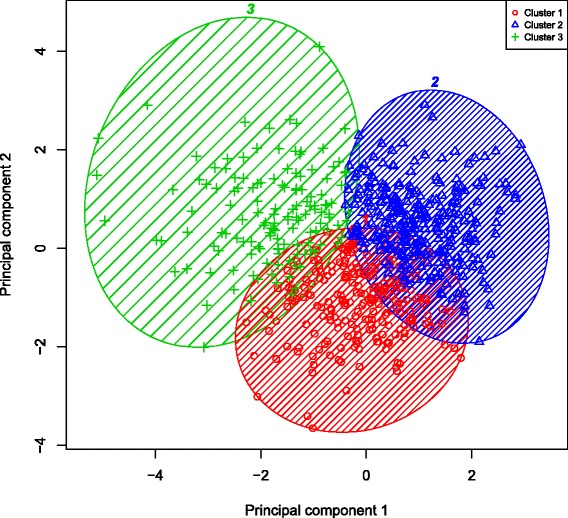
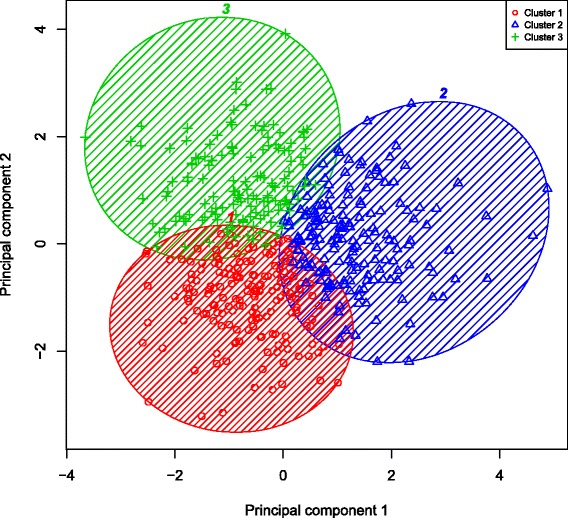
Results: The prevalence of PRISm in COPDGene is 12.3%. Increased dyspnea, reduced 6-minute walk distance, increased percent emphysema and decreased total lung capacity, as well as increased segmental bronchial wall area percentage were significant predictors (p-value <0.05) of PRISm status when compared to control subjects in multivariate models. Although no common genetic variants were identified on GWAS testing, a significant association with Klinefelter's syndrome (47XXY) was observed (p-value < 0.001). Subgroups identified through k-means clustering include a putative "COPD-subtype", "Restrictive-subtype", and a highly symptomatic "Metabolic-subtype".
Conclusions: PRISm subjects are clinically and genetically heterogeneous. Future investigations into the pathophysiological mechanisms behind and potential treatment options for subgroups within PRISm are warranted.
Trial registration: Clinicaltrials.gov Identifier: NCT000608764.
Trial registration: ClinicalTrials.gov NCT00608764 NCT00608764.
Figures
Comment in
-
Concerns about PRISm.Lancet Respir Med. 2022 Jun;10(6):e51-e52. doi: 10.1016/S2213-2600(22)00134-5. Lancet Respir Med. 2022. PMID: 35659007 No abstract available.
References
-
- Swanney MP, Beckert LE, Frampton CM, Wallace LA, Jensen RL, Crapo RO. Validity of the American Thoracic Society and other spirometric algorithms using FVC and forced expiratory volume at 6 s for predicting a reduced total lung capacity. Chest. 2004;126(6):1861–1866. doi: 10.1378/chest.126.6.1861. - DOI - PubMed
-
- Washko GR, Hunninghake GM, Fernandez IE, Nishino M, Okajima Y, Yamashiro T, Ross JC, Estepar RS, Lynch DA, Brehm JM, Adnriole KP, Diaz AA, Khorasani R, D’Aco K, Sciurba FC, Silverman EK, Hatabu H, Rosas IO, COPDGene Investigators Lung volumes and emphysema in smokers with interstitial lung abnormalities. N Engl J Med. 2011;364(10):897–906. doi: 10.1056/NEJMoa1007285. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
